Background
Obstructive sleep apnea (OSA) is a prevalent disorder and well-established risk factor for cardiovascular disease, myocardial infarction, stroke, and increased mortality. Although continuous positive airway pressure is considered the gold-standard treatment, long-term adherence is unsustainable for many patients. As a result, these patients often seek surgical treatment for their condition. Uvulopalatopharyngoplasty (UPPP) has been offered as a treatment option for OSA since it was first pioneered by Dr. Fujita in 1981. Our purpose is to review the evidence for UPPP in OSA.
Best Practice
There is level 1 evidence that suggests UPPP surgery is an effective treatment for OSA in the appropriately selected patient. It is recommended that an anatomy-based staging system be used in place of a severity-based staging system to predict surgical success. Patients with lower anatomy-based stages consistently demonstrate the greatest likelihood of success with UPPP alone (Laryngoscope. 2017;127:2201–2202).
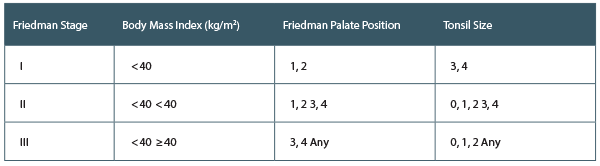
Friedman’s Anatomy-Based Staging System
In 2002, Friedman et al. conducted a retrospective analysis of 134 patients who underwent UPPP for treatment of OSA to validate an anatomy-based staging system (Otolaryngol Head Neck Surg. 2002;127:13–21). Patients were staged based on their Friedman palate position, tonsil size, and body mass index (BMI). Success rates for Friedman stages I, II, and III were 80.6%, 37.9%, and 8.1%, respectively. The authors found their staging system to be an effective predictor of UPPP success. They also proposed that UPPP was effective for stage I patients but counseled against UPPP alone in stage III patients.