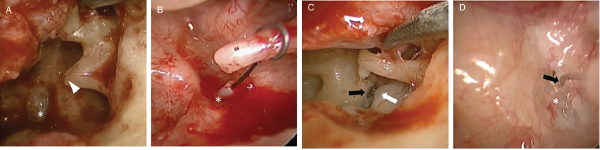
Fig. 1. Intraoperative findings. (A) Necrosis of long process of incus (arrowhead) resulting in prosthesis displacement from stapes footplate (*) (patient 2). (B) Prosthesis displaced to posterior rim of footplate (*) (patient 1). (C) Prosthesis displacement (removed) with prolapsed facial nerve (white arrow) and prominent bony overhang (black arrow), which was drilled to allow for prosthesis placement during revision surgery (patient 3). (D) Short wire loop prosthesis (black arrow) making poor contact with stapes footplate (*) (patient 4).