Operative Technique
Explore This Issue
July 2022Visualization can typically be performed with a standard 0- or 30-degree endoscope for all aspects of the IMAP procedure. The anterior and central aspects of the left and right inferior meatuses are injected with 1% lidocaine with 1:100,000 epinephrine using a 25-gauge needle. Injection is meant to induce vasoconstriction as well as hydrodissect the adherent inferior meatus tissue from the underlying maxilla bone.
Following this, the inferior meatal pocket is elevated (see supporting video). A 7200 Beaver blade is used to make a curvilinear incision at the piriform aperture edge just before the axilla attachment of the ITs. The piriform aperture edge typically sits within 1 to 2 mm posterior to the mucocutaneous junction. Hemostasis is facilitated by the use of quar – ter-inch by quarter-inch micropledgets soaked in 1:1,000 epinephrine. A Rhoton #3 or duckbill elevator is then used to elevate a full-thickness, submucoperiosteal flap, creating a sizable pocket between the inferior meatus mucosa and the lateral nasal wall bone. This pocket is elevated posteriorly to a length of about 3.0 to 3.5 cm, or just proximal to the hard:soft palate junction. Importantly, limited dissection of the adjacent nasal floor is performed, such that the dome of the implant projects medially from the bony sidewall into the airway to simulate normal turbinate architecture rather than the implant sinking medially toward the nasal floor and crowding the airway. Meticulous hemostasis of the submucoperiosteal pocket is important to obtain at this point, and can be achieved with topical hemostatic agents such as epinephrine pledgets or thrombin-infused hemostatic matrix.
Intact, cylindrical cadaveric rib graft (>3.0 cm in length) is then thawed in dilute betadine/saline solution and prepared for implantation on a sterile cutting board. Using a #22 blade, the rib is bisected into two half cylinders, one for each side. Then the graft is whittled down in all dimensions to maintain the half-cylinder shape that will fit within the pocket dimensions required for each ENS patient. Typically, one implant measures 2.5 to 3.2 cm in length, 5 to 6 mm in width, and 6 to 8 mm in height in the setting of IMAP following near-total turbinectomy.
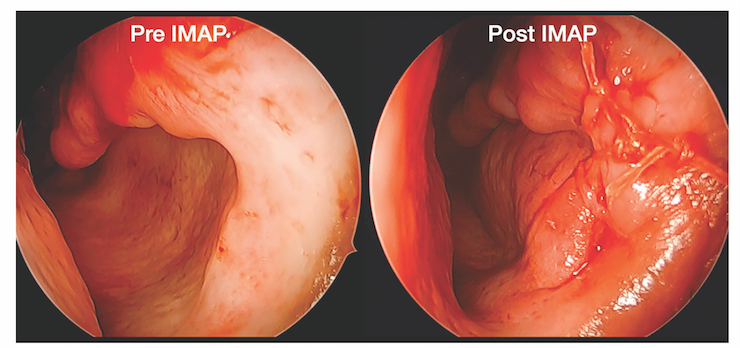
Figure 1. Placement of properly sized, cadaveric rib implant within the submucoperiosteal pocket to augment the left inferior meatus and recreate the rounded, natural contour of a native inferior turbinate projecting from the lateral nasal wall. The incision is then closed using 4-0 Vicryl suture; of note, a 1 to 2 mm airspace between the septum and IMAP graft is maintained for nasal breathing.