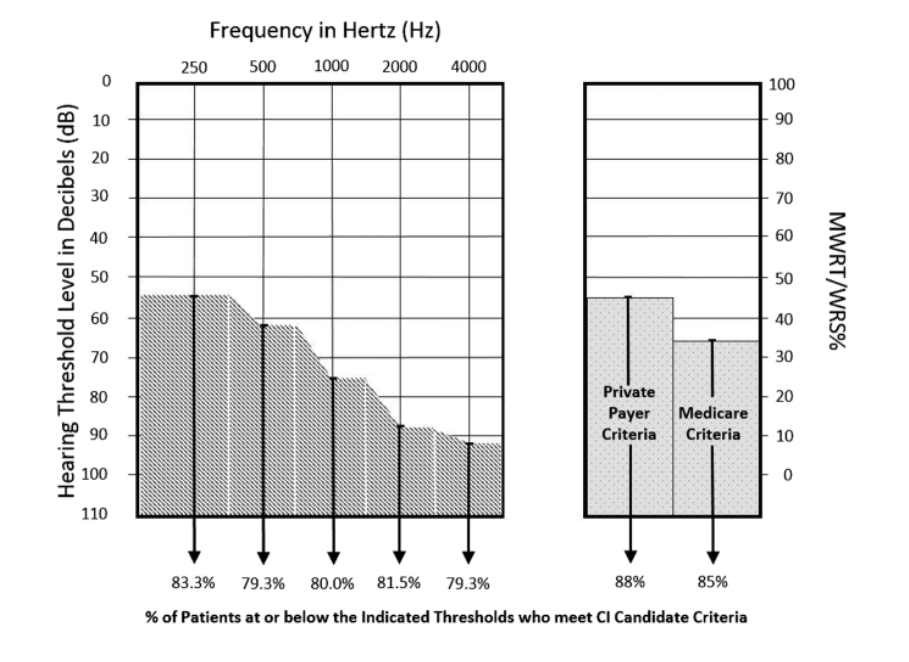
Figure 1. Summary showing the pure-tone and MWRT threshold values that significantly correlated with meeting candidacy requirements upon cochlear implant evaluation. The percentile scores in the bottom row represent the number of patients in the study cohort testing at or below the audiometric measure thresholds shown who then qualified for cochlear implantation. For pure-tone measures, the threshold values were generated through correlation with sentence-level discrimination testing using AzBio in quiet conditions and assuming Medicare candidacy criteria (40% or worse on sentence level discrimination tests). For the MWRT, the threshold values were generated through correlation with sentence level discrimination testing regardless of the type of material used (AzBio in quiet, AzBio in noise, or HINT in quiet). CI = cochlear implant; HINT = Hearing in Noise Test; MWRT = monosyllabic word recognition test; WRS = word recognition score.
Credit: Laryngoscope