Background
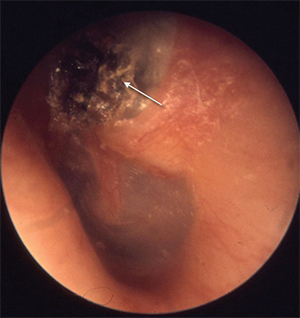
Cholesteatoma
© Welleschik/Wikipedia
Cholesteatoma can be a difficult disease to treat because the underlying cause of the disease, Eustachian tube dysfunction, is generally not addressed. This can lead to recurrent disease. Surgical resection of cholesteatoma can also be quite challenging, and residual cholesteatoma is often present after surgery.
Explore This Issue
February 2017The term recidivism is frequently used to describe both recurrent and residual cholesteatoma. The total recidivism rate has been found in various studies to be between 10% and 70%. The primary treatment has been debated for decades, with recommendations for canal wall down (CWD), canal wall up (CWU), staged procedures, and endoscopic procedures. Historically, CWD procedures have lower overall recidivistic rates. CWU with second-look procedures have similar recidivistic rates.
Recently, some have advocated foregoing the second look in favor of a planned single-stage procedure with CWD procedures for those with known extensive disease, and CWU procedures for those whom the cholesteatoma can be removed completely. The reasoning is that only residual disease is addressed by second-look procedures; if the disease is entirely removed in the primary procedure, second-stage procedures should not be necessary. To minimize any unnecessary procedures, some surgeons recommend two-stage procedures only when cholesteatoma persistence is uncertain. As a response, our group asks this question: “Is a second stage necessary to treat cholesteatoma in canal wall up procedures?”
Best Practice
Second-look procedures keeps overall recurrence from residual cholesteatoma rates similar to that of CWD procedures. In the four studies presented here, 1,250 patients were treated with CWU procedures and 49 (3.9%) unexpected residual cholesteatomas were found. Four hundred seventy-eight planned second-look procedures were performed and 156 (32.6%) residual cholesteatomas were found. Therefore, more than 67% of the second-look procedures were unnecessary.
Finally, new methods, such as nonecho planar imaging magnetic resonance imaging (MRI) for evaluation of postoperative ears, offer highly sensitive and specific evaluation of recurrent and residual cholesteatoma. Use of this imaging modality may help prevent unnecessary surgery for patients when there is concern for residual or recurrent cholesteatoma.
Recently, many have favored a tailored approach, with a second look reserved for those patients when cholesteatoma was thought to be left behind at the primary surgery.
The studies presented here show that a selective approach to staging cholesteatoma surgery, in both adults and pediatric patients, is effective and appropriate and will reduce unnecessary procedures (Laryngoscope. 2016;126: 1499–1500).