The benefits of bilateral hearing include improved speech understanding, especially in background noise; improved localization; and enhanced safety due to increased awareness of the auditory environment.
Explore This Issue
November 2017Although unilateral cochlear implants generally provide good speech understanding under quiet conditions, patients frequently report difficulty understanding speech and speech localization in noisy environments (Curr Opin Otolaryngol Head Neck Surg. 2009;17:351-355).
In addition, “patients with bilateral implants report being less fatigued with the act of hearing at the end of the day,” Dr. Lalwani noted. “A person with a single CI is pretty tired at the end of the day—they have to expend a lot of energy to understand” their environment.
In general, simultaneous bilateral implants are more commonly performed in children than adults. “Children are lifelong learners, but their environment is very compromised in school with a lot of background noise,” Dr. Lalwani said.
Adults often present with different amounts of hearing loss in each ear. “Typically, we will choose to implant the poorer-hearing ear. If the patient gets good benefit, and particularly if the second ear does not benefit from amplification, we will often consider a second side implant,” Dr. Tucci said.
“If there is some residual hearing [substantial low-frequency residual hearing] in the contralateral ear, that ear is managed with a hearing aid,” Dr. Buchman added. “In most cases, the implant and hearing aid together are better than a cochlear implant alone. However, when people recognize that the hearing aid is not providing a lot of value and they are struggling substantially, that is when we consider a second cochlear implant.”
“Most insurers are agreeing to pay for bilateral cochlear implants, but the cost effectiveness of bilateral implantation is not easy to prove, not because patients do not benefit, but because we don’t have accurate ways of measuring either the deficits without a second side CI or the benefits of bilateral implantation,” Dr. Tucci said.
When CROS Is a Better Option
Bilateral cochlear implants are ideal for patients with bilateral deafness, but when having two cochlear implants is not an option, patients may benefit from Contralateral Routing of Signal (CROS) to a cochlear implant, Dr. Buchman noted. This device is indicated for patients with a single cochlear implant and profound hearing loss in the unimplanted ear. The CROS microphone is placed on the unimplanted ear, which delivers sound wirelessly to the cochlear implant, creating access to sounds otherwise not available.
The CROS device and bilateral cochlear implants have not been directly compared. But the CROS system’s microphone is not directly stimulating the ear, Dr. Tucci noted; instead, “it routes the sound to the other [implanted] ear. One would think that directly stimulating the ear would be a better situation. Probably less ideal, but still beneficial.”
Changes in Technology
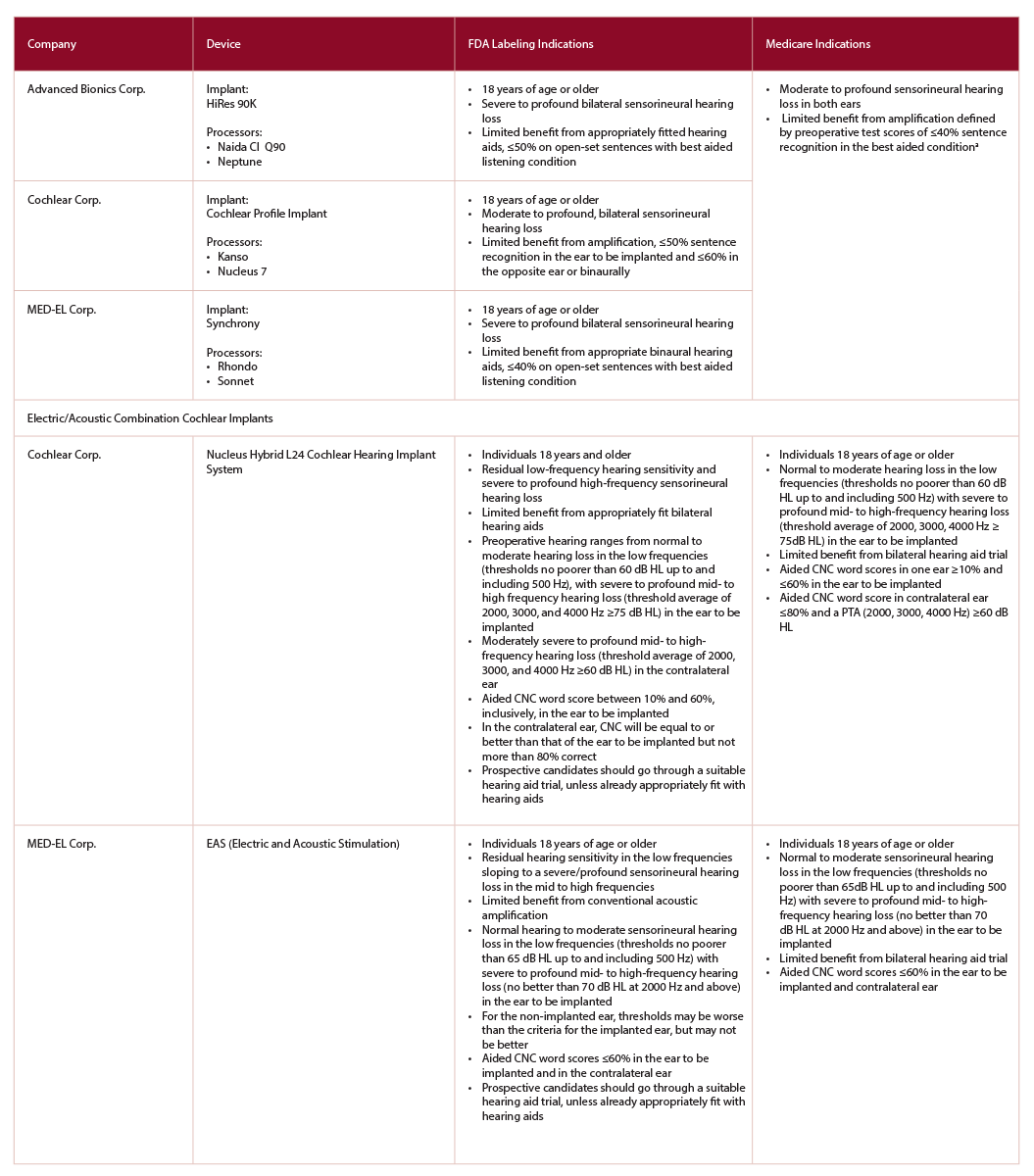
(click for larger image) Table 1: Comparison of Cochlear Implant Candidacy between FDA-Approved Devices and Medicare Adult Criteria
CMS, Centers for Medicare & Medicaid Services;
CNC, consonant-vowel nucleus-consonant;
FDA, Food and Drug Administration
a Medicare is considering expanding criteria to include those individuals with more residual hearing—≤40% sentence recognition in the ear to be implanted and ≤60% in the opposite ear.