 TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope articles free of charge, visit Laryngoscope.com.
TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope articles free of charge, visit Laryngoscope.com.
Explore This Issue
August 2016Background
(click for larger image)
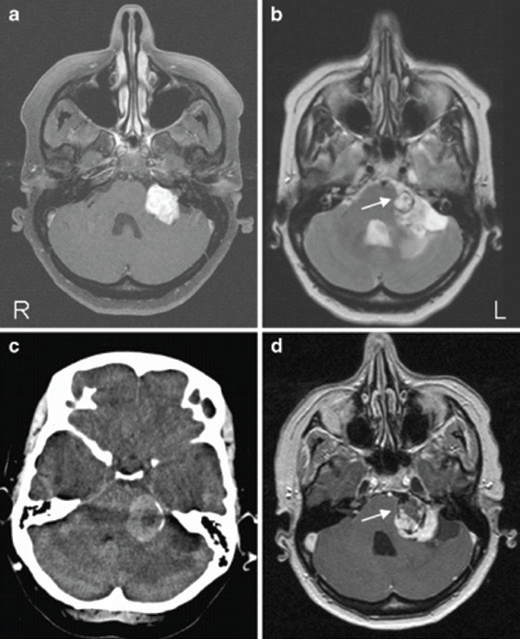
Caption: A) Axial T1-weighted MRI with gadolinium contrast enhancement showing left-sided vestibular schwannoma (VS). B) Axial T2-weighted MRI of the posterior fossa showing round lesion inside the VS (arrow) with surrounding hemosiderin deposits. C) Axial CT image through the posterior fossa showing a hyperdens area due to intratumoral hemorrhage in the VS. D) Axial T1-weighted postcontrast MRI showing hemorrhage (hypo-intense area) inside lesion (arrow). The VS enhances homogeneous and contrast-sparing occurs at the location of the hematoma (R right, L left).
Gadolinium contrast enhanced T1 weighted magnetic resonance imaging (GdT1W MRI) is the most widely accepted evaluation for asymmetric sensorineural hearing loss (ASNHL). It has replaced auditory brainstem response (ABR) and computed tomography to detect anatomical abnormalities such as acoustic neuromas (ANs) as the initial screening test after obtaining the history, physical, and audiogram. The cost of a complete brain GdT1W MRI is not insignificant. Gadolinium has a risk of nephrogenic systemic fibrosis and must be used cautiously with renal dysfunction. Alternatively, noncontrasted fast spin-echo T2-weighted (FSE T2W) MRIs focused on the internal auditory canal (IAC) and cerebellopontine angle (CPA) can be performed in only 10 minutes. The sensitivity of these protocols for screening, particularly for smaller lesions, has been questioned. Disagreement exists regarding the cost-effectiveness and necessity of an initial GdT1W MRI, which is relevant in an era needing cost-containment.
Best Practice
Nonenhanced FSE T2W MRI targeted to the IAC/CPA can be used as an initial imaging modality to rule out anatomical abnormality in ASNHL because of the excellent detail it provides. It is rapid, cost-effective, and sensitive. To be appropriate and accurate, it requires patient evaluation by an experienced otolaryngologist, slices ≤ 2 mm, and review by a neuroradiologist. It should be applied judiciously to patients without other neurologic or vestibular symptoms. Otolaryngologists need to remain aware and counsel their patients that small ANs, labyrinthine ANs, and inflammatory disorders can be missed. It is crucial to have open communication between the otolaryngologist and neuroradiologist to ensure proper protocoling. The otolaryngologist should begin this by communicating that the MRI is ordered to evaluate for ASNHL; this is different than the widely accepted protocol with contrast. This will enable the neuroradiologist to evaluate the MRI appropriately and recommend further imaging with contrast to clarify positive findings or inadequate studies. Since the T2W screen can either reliably identify a mass or prompt the use of contrast, it is a safe and effective screening tool. The benefit could be realized in substantial time and cost savings for the patient and medical system (Laryngoscope. 2015;125:783-784).