Explore This Issue
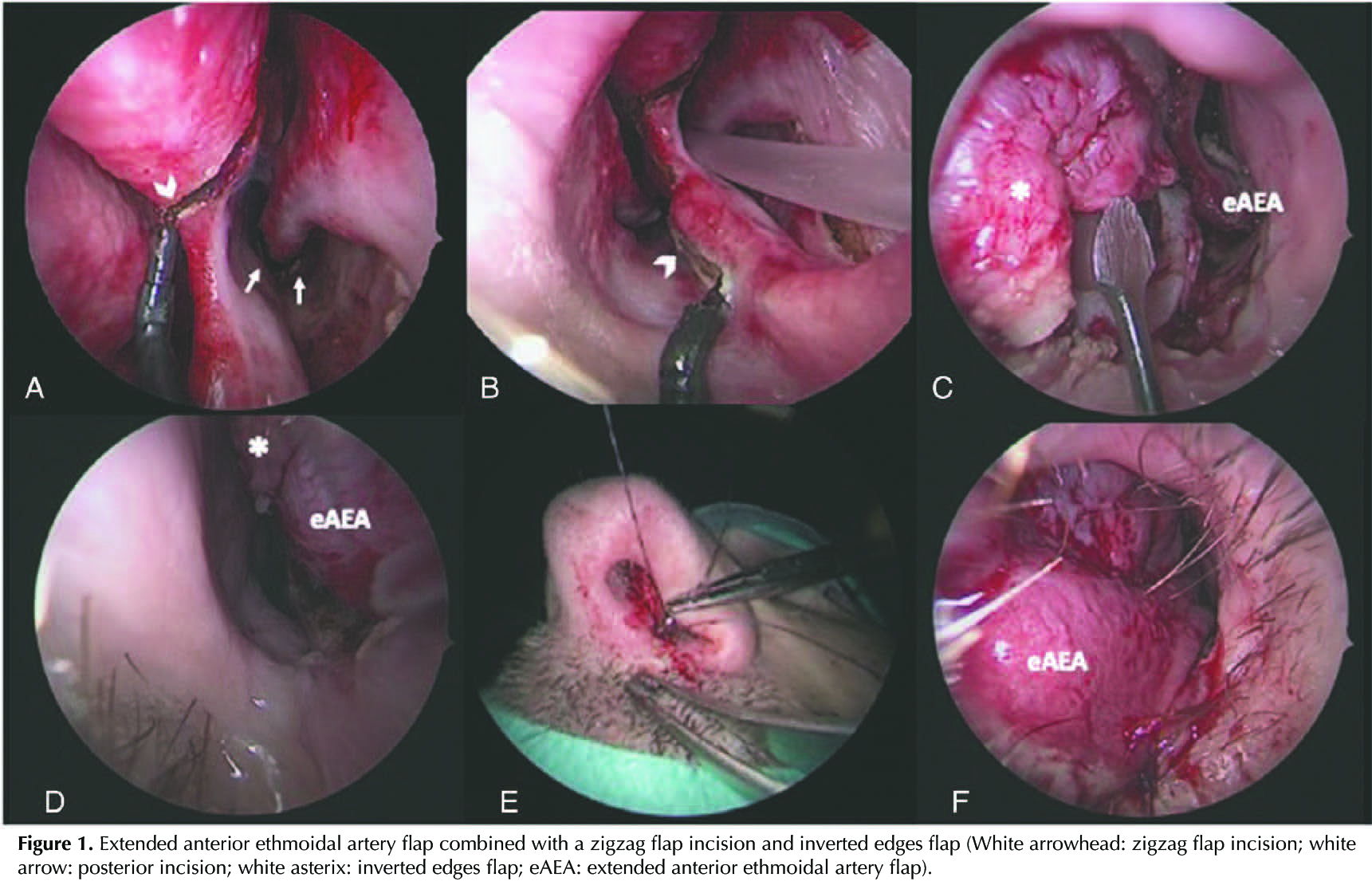
May 2023Once the SP edges are turned, and the size of the perforation has decreased at the expense of its most superior and anterior edge (Figures 1D, 1C), the PEF is rotated and placed until the perforation and the inverted edges are completely covered (Figures 1F, 1D). Two stitches are placed in the most anterior and superior part of the flap (Figure 1E). Silicone nasal splints are fixed to the columella for three to four weeks.
RESULTS
Four patients from Centro Médico Teknon and Hospital Clinic of Barcelona were included in this study. The mean age was 43 years. The cause of the SP was secondary to drug abuse (cocaine) in three cases and nose picking in one patient. An eAEA was used in three cases and GPA was performed in one patient due to the posterior edge of the SP being anterior to the incisive channel. All the patients had a complete closure of the perforation six months after surgery.
Although this is a small case series and the follow-up time was only up to 13 months, our results show that the use of EE in combination with the anterior zigzag incision for PEF can be useful tools that could be considered when performing a surgical closure of anterior SP. This technique is limited to SP with osseocartilaginous support and a complete epithelialization of the perforation margins.