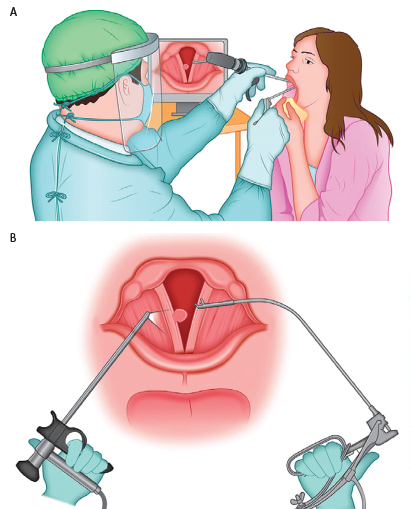
Figure 1. A) Operative setting for the procedure. The surgeon, wearing personal protective equipment, is observing the procedure on the monitor, maintaining adequate distance from the patient. The patient is seated as for routine otolaryngologic examination and is holding the tongue in a gauze. B) Schematics of the procedure. Curved microforceps for indirect laryngeal operations, held in the surgeon’s right hand, is aiming for the lesion of the right vocal fold, under the visual guidance of the rigid telelaryngoscope held in the surgeon’s left hand.