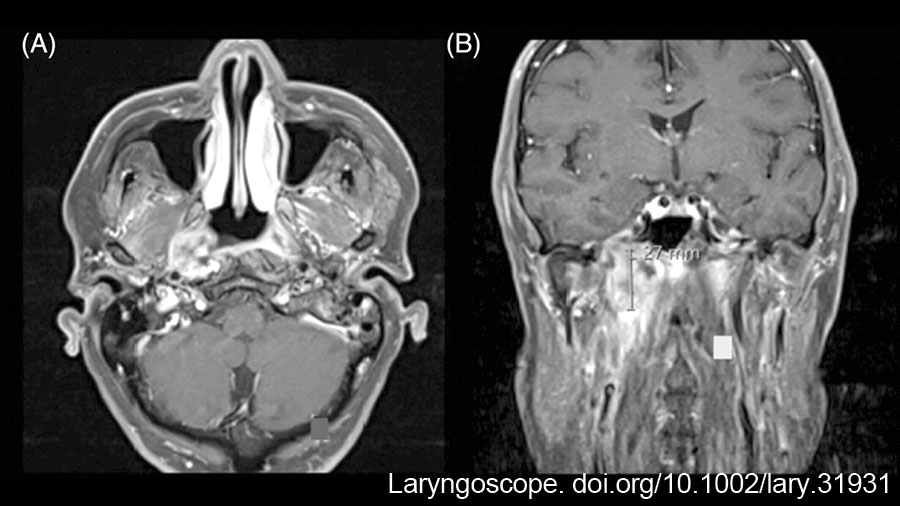
Figure 1: (A) T1-weighted MRI with gadolinium and fat saturation in the axial plane: Enhancing nasopharyngeal lesion centered in the right fossa of Rosenmüller, with extension to the prevertebral fascia, parapharyngeal ICA, and pterygoid plates; (B) Coronal plane: Enhancing right nasopharyngeal lesion, with extension superiorly into the mandibular strut of the greater sphenoid wing and foramen ovale, and laterally into the ITF and parapharyngeal space. ICA, Internal carotid artery; ITF, Infratemporal fossa. doi.10.1002/lary.31931
An SMIF was then harvested for reconstruction in the manner described by Patel and colleagues. (Laryngoscope. doi.org/10.1097/01.mlg.0000246519.77156.a4). The nasopharyngectomy defect was inspected and measured; a 4 × 6 cm skin paddle was designed in the submental skin. Subplatysmal flaps were previously raised in the neck dissection, and the marginal mandibular nerve was identified and mobilized superiorly. The submandibular gland was dissected from its fascial capsule and excised to allow identification of the facial and submental vessels (Fig. 2A). The anterior skin paddle incision was carried to the superficial layer of the deep cervical fascia. The integrity of the vascular pedicle was confirmed, and the skin paddle incision was completed. The flap was harvested from left to right (distal to proximal) by identifying and transecting the mylohyoid muscle in the midline and dividing the right anterior belly of the digastric muscle from the mandible and hyoid. The mylohyoid was then detached from the mandible and hyoid. The muscle was bluntly dissected from the middle layer of deep cervical fascia to mobilize the vascular pedicle (Fig. 2B). The facial artery and vein were ligated above the origin of the submental vessels, and the pedicle was dissected proximally to maximize its length (Fig. 2C). The parapharyngeal space had been exposed during tumor resection as the MPM was detached from its origin by drilling the pterygoid plates. Access to the parapharyngeal space in the neck was facilitated after dividing the mylohyoid muscle from the mandible during flap harvest. The tunnel for transposition of the SMIF to the nasopharynx was then created by simply releasing the stylomandibular ligament and dilating the parapharyngeal space through blunt dissection along the MPM (Fig. 2D).
Explore This Issue
April 2025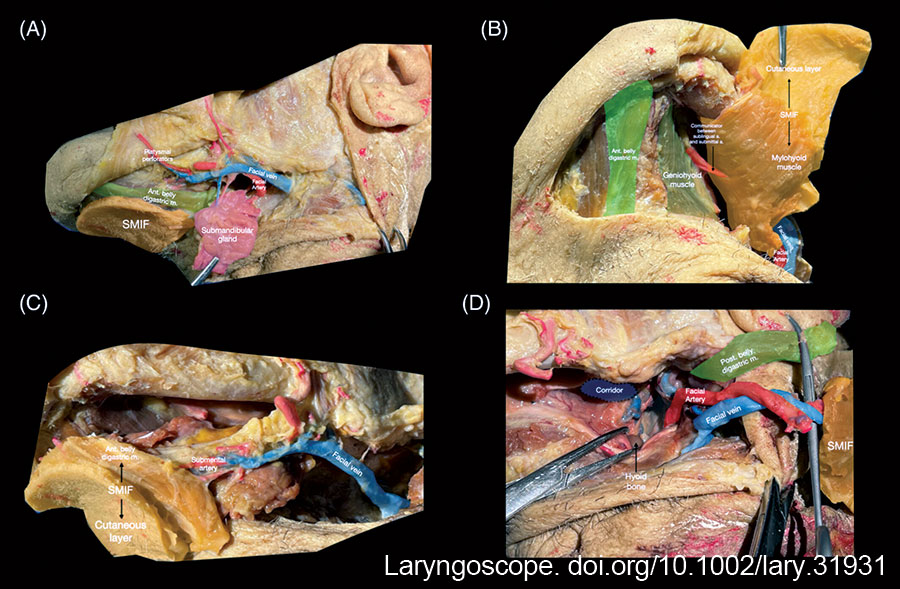
Figure 2: Harvesting the SMIF: (A) meticulous excision of the submandibular gland to preserve the submental vessels; the common facial and external jugular veins are preserved; (B) the mylohyoid muscle is divided at the midline raphe and released from the mandible and the hyoid; the ipsilateral anterior digastric is included to preserve perforating arteries. The flap is then bluntly dissected away from the geniohyoid muscle and middle layer of deep cervical fascia; the mylohyoid is included in the flap; (C) the myocutaneous SMIF may include a sizeable skin paddle along with submental fat and the anterior belly of the digastric muscle and mylohyoid muscle; (D) retrograde dissection of the facial artery to its origin from the external carotid artery maximizes pedicle length. A tunnel is dissected through the parapharyngeal space medial to the mandibular insertion of the medial pterygoid muscle to allow transposition of the flap into the nasopharynx. Ant, Anterior; M, Muscle; Post, Posterior; SMIF, Submental island flap. https://doi.org/10.1002/lary.31931
Leave a Reply