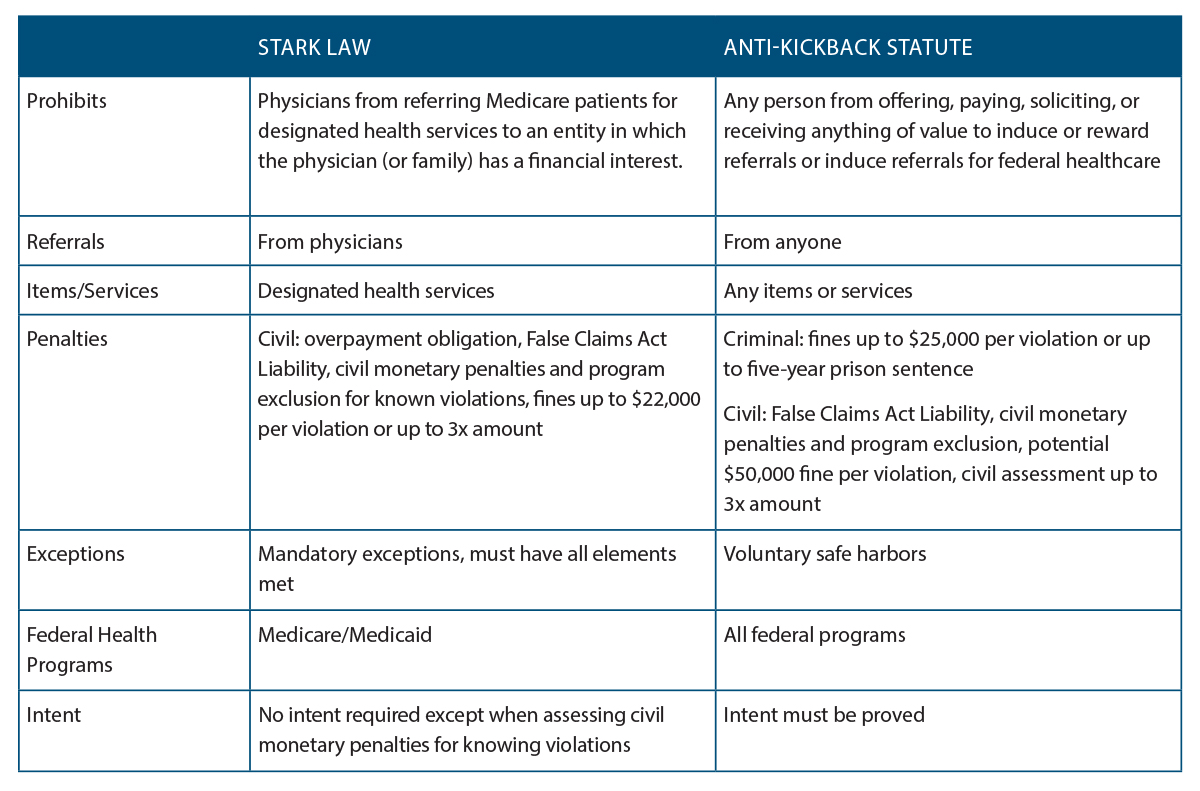
(click for larger image) Key Differences Between the Stark Law & the Anti-Kickback Statute
The CMS and the OIG are proposing four new value-based exceptions or safe harbors:
Explore This Issue
February 2020- Shared Data Services: To improve patient care coordination, a specialty physician practice could share data analytics services with a primary care physician practice.
- Coordinated Patient Discharge: Hospitals and physicians could work together in new ways to coordinate care for patients being discharged from a hospital. The hospital could provide the discharged patients’ physicians with care coordinators to ensure that patients receive appropriate follow-up care and share data analytics to help physicians ensure that their patients are achieving better health outcomes. Remote monitoring technology could also be used to alert physicians or caregivers when a patient needs a healthcare intervention to prevent unnecessary emergency department visits and readmissions to hospitals from which they were discharged.
- Smart Pillboxes: A physician practice could provide smart pillboxes to patients without charge to help them remember to take their medications on time. The practice could also provide a home health aide to teach the patient and caregiver(s) how to use the pillbox. The pillbox could automatically alert the physician practice and caregiver when a patient misses a dose so they could follow up promptly.
- Shared Cybersecurity Software: Hospitals and physicians often share information about their patients, so it’s important to ensure that no weak links compromise patient health or information protected by the Health Insurance Portability and Accountability Act (HIPAA). Under the proposed rules, a local hospital could improve its cybersecurity and the cybersecurity of providers it works with regularly by donating (i.e., free of charge) cybersecurity software to each physician who has access to the hospital’s network in connection with services referred to the hospital. Such software would improve the security measures in place for all users accessing a hospital’s network, minimize the risk of a hacker attack, and prevent hackers from spreading an attack to other physicians and hospitals whose systems are interconnected.
Terms and Concepts
The CMS and the OIG are proposing clarifications to the definitions of fair market value, volume or value, and commercially reasonable in the exceptions provided by the Stark law and the AKS.
Fair Market Value
Many of the Stark exceptions or AKS safe harbors require compensation for any services provided under the contemplated arrangement (e.g., sales and marketing, professional healthcare, billing) to be at fair market value, a concept that varies greatly by the service, geographic location, provider, and other factors. The CMS would define fair market value as “the value in an arms-length transaction, with like parties and under like circumstances, of like assets or services, consistent with the general market value of the subject transaction.” This CMS definition would incorporate the concept of general market value—the price the assets or services would bring as the result of bona fide bargaining between a buyer and seller in the subject transaction on the date of acquisition of the assets or at the time the parties enter into the service arrangement.
In its proposed rule, the OIG acknowledged the difficulty of reconciling the notion of fair market value with value-based arrangements and requested further comments specifically on that concept as a requirement.
Volume or Value
The CMS and the OIG noted that looming penalties may have a chilling effect on models and arrangements designed to reduce overall costs and improve quality of care. That’s because many cost-saving practices relate to patient referrals and shared or free services, which violate the traditional volume or value of referrals prohibitions under both the Stark law and the AKS. The CMS has proposed various revisions to the definition and the development of an objective standard or bright line tests in the proposed rule, which it hopes to finalize after reviewing public comments.
Commercial Reasonableness
The CMS and the OIG are considering how to define an arrangement as commercially reasonable, but disagree about the final language. Both debate whether to even require that value-based arrangements be commercially reasonable.
The CMS put forth two possible definitions for commercial reasonableness:
1) “The particular arrangement furthers a legitimate purpose of the parties and is on similar terms and conditions as like arrangement;” or 2) “The arrangement makes commercial sense if entered into by a reasonable entity of similar type and size and a reasonable physician of similar scope and specialty.”