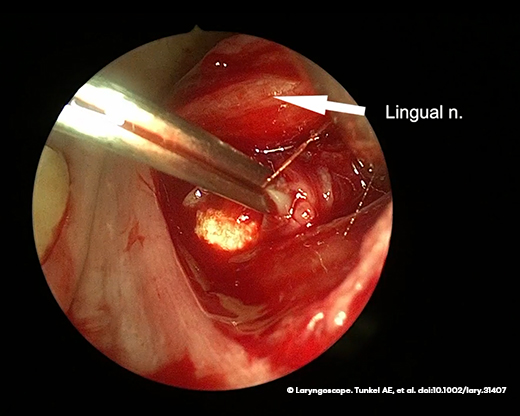
Figure 1. An image from a video demonstrating in-office transoral hilar sialolithotomy showing the stone before extraction.
Informed consent is obtained for all patients. A sweetheart retractor or wooden tongue depressor is utilized to retract the tongue and expose the floor of the mouth. The sialolith is localized using a combination of palpation and ultrasound. Approximately 3 mL of local anesthesia (1% lidocaine with 1:100,000 epinephrine) is injected submucosally into the floor of the mouth to provide anesthesia and accomplish hydrodissection of the superficial tissues. A number 15 scalpel blade is then utilized to make a mucosal incision, and blunt dissection is performed. Care is taken to identify the lingual nerve and mobilize it medially, retracting the nerve away from the field so it remains protected. Lateral and deep to the lingual nerve and deep to the mylohyoid fibers, the submandibular duct and the calculus are identified. The distal-most aspect of the submandibular duct is grasped with forceps, and a scalpel is used to incise the duct in a parallel fashion. Blunt dissection with tenotomy scissors is then used to confirm identification of the sialolith (Figure 1).
Explore This Issue
May 2024Once the stone is retrieved with a curved clamp, ultrasound is performed to confirm no further presence of sialoliths. If the dochotomy is greater than 1 centimeter in length, a sialodochoplasty is then performed. Two 4–0 chromic gut sutures are placed in a simple interrupted fashion to suture the inside of the duct to the posterior floor of the mouth mucosa, marsupializing the duct. A lacrimal probe is placed in the ductal lumen to confirm ductal patency. After the procedure, the patient is instructed to frequently massage the gland to promote salivary flow. They are also encouraged to stay adequately hydrated and use sialogogues if necessary. Patients return for follow-up after one week to ensure ductal patency.
RESULTS
A total of 40 patients met inclusion criteria for this review, having undergone an in-office transoral sialolithotomy for intraglandular or hilar stones between January 2020 and July 2022. Of these patients, 19 were female (47.5%) and 21 were male (52.5%). The average age was 52.8 years. Laterality of stones was relatively balanced, with 21 patients presenting for left-sided symptoms (52.5%) and 19 with right-sided symptoms (47.5%). A total of 55 stones were removed; 94% of removed stones were hilar or intraglandular. On average, patients had 1.45 ± 0.72 stones removed, with a mode of one stone removed per patient. The average stone size was 0.98 ± 0.54 centimeters in the greatest dimension.
Of the 40 attempted in-office sialolithotomies, 36 (90%) were successful. Failure to complete the procedure was due to a vasovagal reaction during the procedure (1), stone adherence to the submandibular duct or gland (2), or poor visualization secondary to patient anatomy (1). Two patients ultimately underwent transoral excision under general anesthesia (Table 1). Only two complications were reported: one patient with temporary lingual nerve paresis and a second with a postoperative intraglandular abscess. Only three (8%) patients experienced recurrence of salivary stones after the in-office procedure.