The strap muscles are elevated as the dissection progresses, exposing the thyroid gland. Again, dissection must be careful, and the monopolar electrocautery should remain in direct contact with the inferior border of the strap muscles to keep a safe distance from IJV. In case of IJV injury, direct ligature or vascular clips (3 or 5 mm) may be used.
Explore This Issue
November 2021Dissection must be pursued until the contralateral omohyoid muscle is reached (Figure 1). Thus, the da Vinci Kuppersmith retractor can be put into place, elevating the skin and creating a workspace sufficient for robotic dissection of both thyroid lobes.
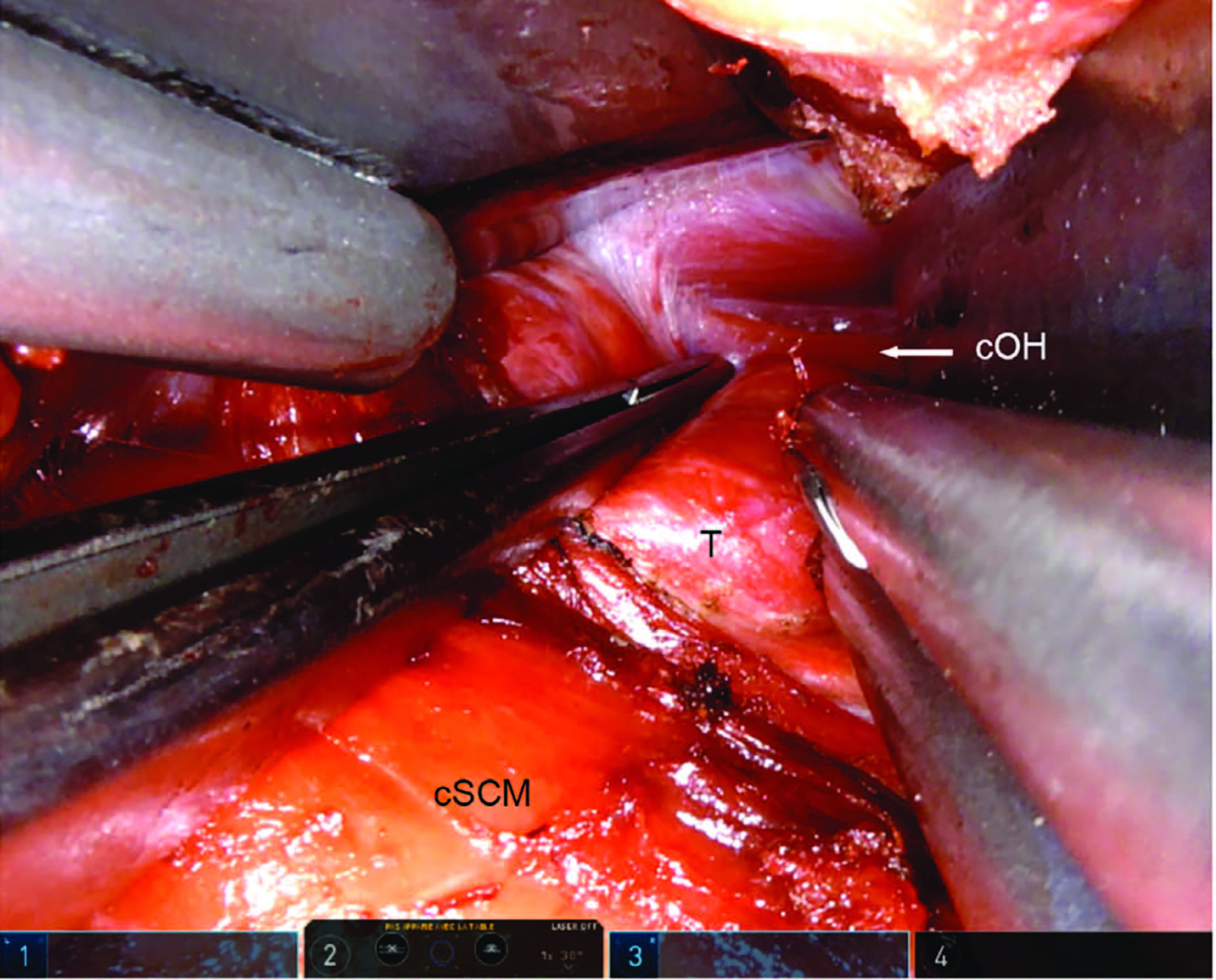
Figure 1. Final view with thyroid and landmarks. Right transaxillary approach. The forceps retracts the thyroid gland downward
to expose the contralateral omohyoid muscle, which is the last landmark to be seen before the final Kuppersmith
retractor is put in place. cOH = contralateral omohyoid muscle; cSCM = clavicular head of the sternocleidomastoid muscle;
T = thyroid gland. SIMON F, ET. AL. LARYNGOSCOPE. DOI:10.1002/LARY.29753
Closure After Robotic Surgery
It is of paramount importance to check the entire workspace for bleeding, especially from the muscle tissue, to prevent hematoma. This is especially true during the first cases of TARS for inexperienced surgeons, when hemostasis may have been undermined during the initial approach. Careful inspection of the muscles under the retractor is necessary as injury can be sustained during the robotic sequence.
Ropivacaine is injected in the wound to facilitate postoperative pain management. No drain is required (no risk of hematoma airway compression as any bleeding seeps into the transaxillary surgical workspace).
Wound closure is done as follows: Vicryl 3-0 suture of the muscle at the level of the clavicle limits dead space in the wound. Skin closure combines Vicryl 3-0 interrupted deep suture and Monocryl 3-0 subcutaneous continuous suture.
RESULTS
Transaxillary procedure was undertaken in 849 patients from 2010 to 2018. Overall complication rate of the transaxillary approach was 2.2% (19 cases), including hematoma, seroma, and transient brachial plexopathy. Hematoma was the main complication (1.5%—13 cases), but none were compressive as they were all located in the transaxillary surgical corridor.
The IJV was injured once (0.12%) and EJV 14 times (1.65%) over the studied period. Bleeding was controlled using surgical clips and did not induce postoperative hematoma.
Concerning the robotic thyroid dissection, complications included 48 cases (6%) of transient hoarseness due to unilateral recurrent laryngeal nerve palsy (spontaneous recovery at the six-week follow-up). Transient hypocalcemia was noted in 87 cases (10%, spontaneous recovery at the one-week follow-up). There were five cases (0.1%) of definitive unilateral palsy and three cases (0.1%) of definitive hypocalcemia (3/5 and 2/3 in cancer patients, respectively). There were two chyle leaks, and no esophageal or tracheal perforations.