INTRODUCTION
As a surgical procedure to implant an electronic medical device, cochlear implantation is subject to not only complications related to open procedures, but also those related to device failure, implant migration, and off-target stimulation, among others. Device migration remains one of the more common complications of cochlear implantation, and a variety of surgical techniques have been developed to fix cochlear implants (CIs) in place (Otol Neurotol. 2021. doi:10.1097/MAO.0000000000003108). Improvements in device design and surgical techniques have resulted in a reduction in surgical cochlear implant revision rates (2.9% from 6%) over the past two decades (Otol Neurotol. 2021. doi:10.1097/MAO.0000000000003108; Laryngoscope. 2020. doi:10.1002/lary.28071).
Explore This Issue
March 2024Broadly, fixation methods can be divided into the bony-bed technique, in which a bone well is drilled into the calvarium to accommodate device placement, and the tight periosteal pocket technique, which fixes the device under blunt-elevated pericranium. Either technique can be modified with suture tie-downs, historically either in drilled channels in the cranial cortex, or directly to the periosteum (Otol Neurotol. 2021. doi:10.1097/MAO.0000000000003108). A systematic review comparison of these techniques did not demonstrate a significant difference in implant migration rates between the two general categories, but tie-down techniques were not included in the comparison (Otol Neurotol. 2021. doi:10.1097/MAO.0000000000003108). Single-center studies of a bony well technique with bone-channel suture tie-down report very low revision rates (two devices in 1,065 devices total) (Otol Neurotol. 2017. 2021. doi:10.1097/MAO.0000000000001302) and significantly lower migrations compared with periosteal pocket techniques (J Laryngol Otol. 2018. doi:10.1017/S0022215118000609).
In this study, we describe a time-saving modification of a bony-bed technique that utilizes screw-fixated Mersilene cervical cerclage suture, originally designed for treatment of uterine cervical insufficiency, as a simple, quick, and effective method for tie-down receiver/stimulator fixation. In our series, this modification of a tie-down technique resulted in no revision surgeries for receiver/stimulator migration, without longer operative times.
METHOD
Surgical Technique
Cochlear implantation technique was performed by a standard postauricular mastoid approach. A #4 cutting burr was used to drill a seat for placement of the implant. A trough was then drilled from the seat to the mastoid. The anterior edge of this seat was approximately 8–10 mm from the posterior edge of the mastoid.
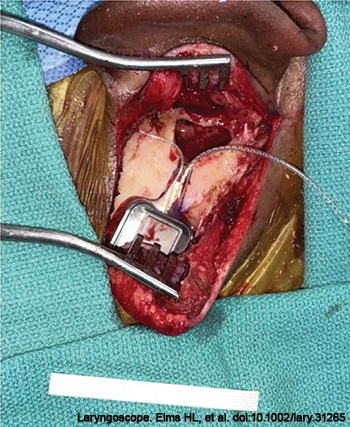
Figure 1. The cochlear implant is placed in the seat and trough; cervical cerclage tape is displayed on the drape.
The implant was opened and positioned in the drilled seat, with electrodes oriented anteriorly toward the planned cochleotomy (Figure 1). One-quarter-inch cervical cerclage tape was draped superoinferiorly across the implant receiver/stimulator and tightly secured to the bone with two 4-mm self-tapping titanium screws (Figure 2). With the implant receiver/stimulator secured, either a cochleostomy or atraumatic round window insertion was performed. This technique can be used to secure the receiver/stimulator of any of the available cochlear device brands.