INTRODUCTION
Explore This Issue
March 2026The middle meningeal artery (MMA) originates from the maxillary artery, a branch of the external carotid artery, and enters the skull base through the foramen spinosum from the infratemporal fossa. It plays a crucial role in supplying blood to various intracranial structures and the calvarium. The MMA is frequently encountered during surgical procedures involving the infratemporal fossa either via an endonasal endoscopic approach or an infratemporal fossa approach. Incidental bleeding from the MMA is usually profuse and sometimes difficult to control, especially if it happens during a surgical approach to the infratemporal fossa via an endonasal endoscopic approach. Moreover, it can be mistaken for bleeding from the nearby horizontal petrous internal carotid artery (ICA) due to its proximity.
Here, we present a case in which we successfully removed a giant cell tumor in the infratemporal fossa via an infratemporal fossa approach after selectively embolizing the MMA during transfemoral carotid angiography. During the infratemporal fossa approach, the embolized MMA was a useful surgical landmark to confirm the posterior boundary of the tumor with minimal bleeding during surgery.
MATERIALS AND METHODS/PATIENT INFORMATION
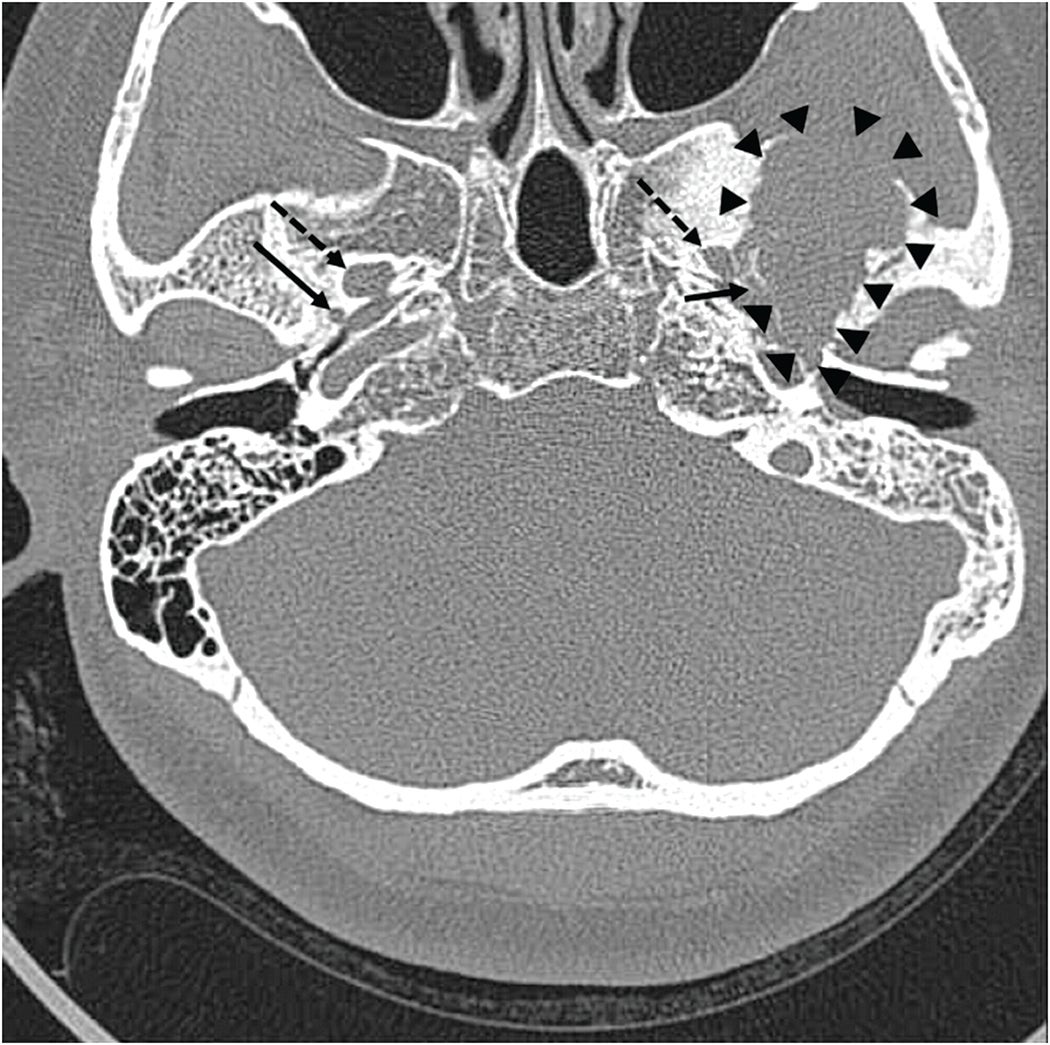
Figure 1. Pre-operative computed tomography showing a giant osteolytic lesion (margin indicated with arrow heads) contacting foramen spinosum (solid arrows), but not in contact with foramen ovale (dashed arrows).
A 46-year-old woman presented with persistent middle ear effusion and hearing loss on the left side. Pain during mastication started approximately five years prior and had recently gotten worse with trismus. She also presented with parageusia and a sour taste. Otoscopic examination revealed middle ear effusion on the left side, and she could not inflate the middle ear by Valsalva maneuver. A pure tone audiogram revealed conductive hearing loss on the left side. She underwent ventilation tube insertion in her left ear, but the tube was noted to have fallen out at an outpatient follow-up visit 30 months later, with recurrence of the middle ear effusion. There was no mass lesion on endoscopic nasopharyngeal examination. Therefore, Eustachian tube balloon dilatation was planned, and a pre-operative computed tomography (CT) scan was performed. High-resolution CT scans revealed a large, ill-defined osteolytic lesion with adjacent sclerotic changes in the left middle cranial fossa (Figure 1, arrowheads). Magnetic resonance imaging (MRI) showed the tumor did not contact the foramen ovale but was adjacent to the foramen spinosum and mandibular condyle. MRI showed an approximately 4-cm heterogeneous mass in the left temporal bone involving the sphenoid bone and left temporomandibular surface, growing downward into the infratemporal fossa. The mass appeared as an iso-and low-signal mixed lesion on pre-contrast T1-weighted images, and there was a markedly low signal within the tumor on T2 imaging with cystic changes. Post-contrast T1-weighted images revealed a heterogeneous enhancing lesion with intense enhancement of cystic areas, which is highly suggestive of a giant cell tumor. Positron emission tomography (PET) revealed a strong signal of high accumulation of 18F-fluoro-2-deoxy-D-glucose (18F-FDG) in the infratemporal fossa.
SURGICAL TECHNIQUE AND RESULTS
Surgical removal of the giant cell tumor was conducted using an infratemporal fossa approach type B. The day before surgery, embolization of the left MMA was performed. Briefly, right common femoral artery access was obtained using a 5-French micropuncture kit, and common carotid and external carotid angiography were performed using a standard 4-French diagnostic catheter. After super-selecting the left accessory MMA with a microcatheter (Excelsior SL-10; pre-shaped 45″; Stryker Corp., Kalamazoo, MI, USA) and a microwire (Synchro-14; Stryker Corp.), embolization was performed using a detachable coil. A temporal bone CT scan confirmed that the MMA was successfully occluded.
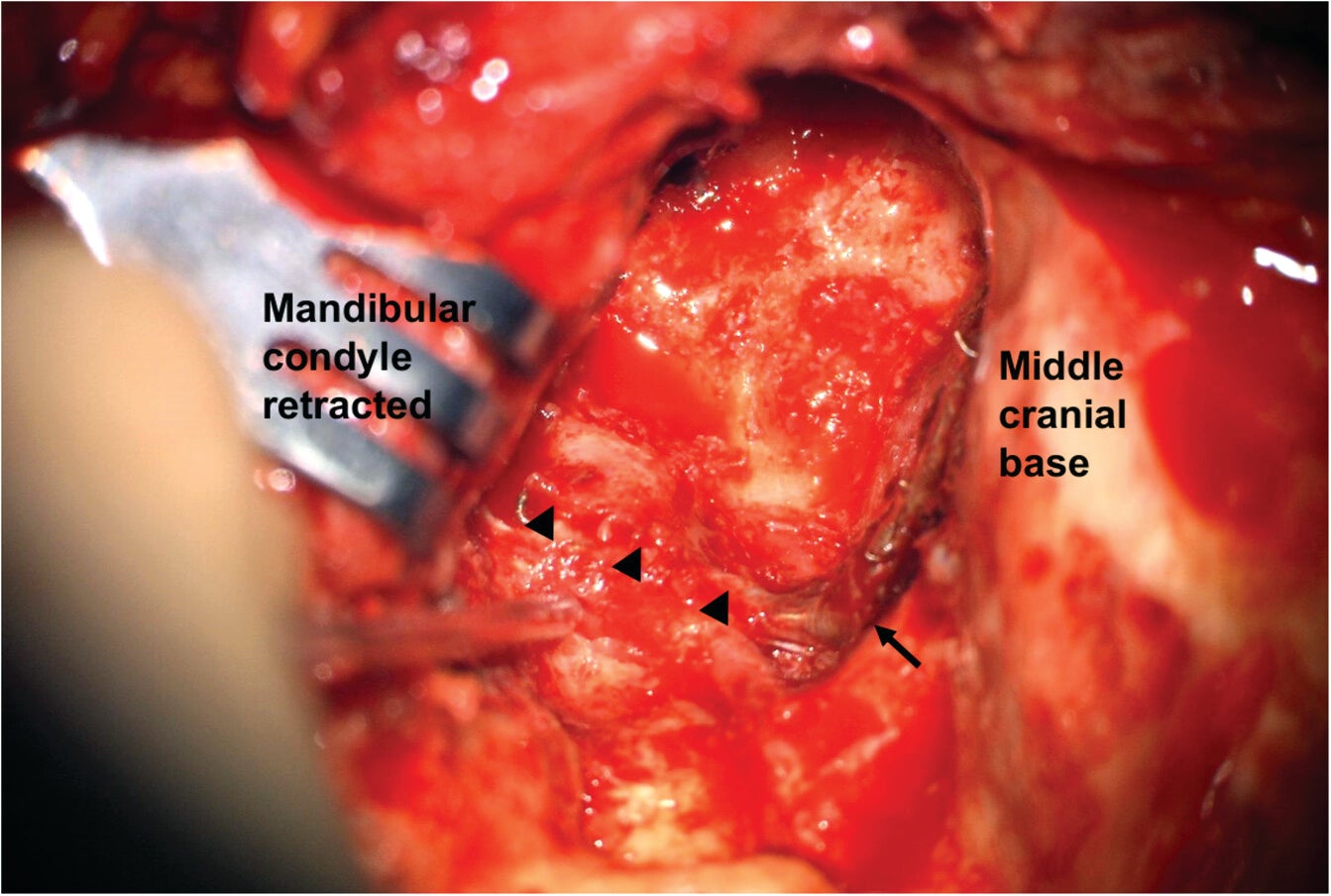
Figure 2. Exposure of the infratemporal fossa. The middle meningeal artery (arrow heads) is lying below, entering the skull base through the foramen spinosum (arrow). The mandibular condyle is retracted.
A large C-shaped postauricular incision was designed, and the flap was elevated superficially to the temporalis muscle. The external auditory canal was closed by meatal skin, and a subtotal petrosectomy was done. The temporalis muscle was reflected, the zygomatic arch was removed and preserved, and then the mandibular condyle was retracted downward to expose the infratemporal fossa. Following substantial removal of the tumor mass using an ultrasonic aspirator in the infratemporal fossa, an embolized coil in the MMA was identified in the medial border of the tumor.
The internal carotid artery and the Eustachian tube were identified inferior to the embolized MMA. Bleeding remained minimal during the procedures. By using the coil in the MMA as a surgical marker, we accurately identified and confirmed the posterior medial boundary of the tumor, facilitating precise tumor removal (Figure 2). Abdominal fat was used to obliterate the dead space, and the skin was closed.
CONCLUSION
Selective embolization of the MMA prior to removal of a giant cell tumor located in the infratemporal fossa allowed us to successfully complete the surgery with minimal bleeding. The embolized MMA also served as a helpful surgical landmark to accurately identify and confirm the boundary of the tumor. Additionally, embolization of the MMA is expected to be useful in endoscopic skull base surgeries, given its potential to reduce hemorrhage and enhance precision in a narrow field of view. In addition, the role of FDG-PET has not been emphasized before, but it was quite a useful imaging method in the diagnosis and follow-up of the giant cell tumor in this case.
Leave a Reply