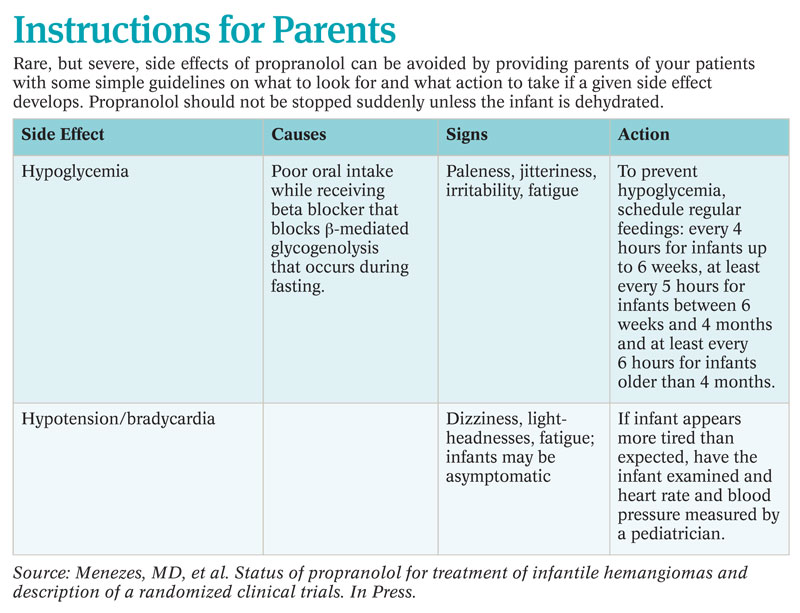
“Parents should always be counseled that they need to feed babies on a regular basis, and if the baby is missing a meal for whatever reason, then the propranolol dose should be withheld until the baby resumes eating,” she said.
Explore This Issue
July 2011Other infants in whom propranolol should be used with caution include those with reactive airway disease or heart problems. Dr. Buckmiller recommended not using propranolol in these patients, whereas others suggested that propranolol can be used with caution.
Dianne Atkins, MD, a pediatric cardiologist at the University of Iowa Children’s Hospital in Iowa City, said propranolol has been used extensively and safely in children to treat a number of cardiac problems, such as hypertension, arrhythmias and congenital heart disease. However, she did caution that bradycardia may occur, particularly in premature infants or in those younger than six months, and may require reducing the propranolol dose.
Overall, Dr. Atkins emphasized the need for close monitoring when infants begin treatment. She admits infants younger than six months for at least 24 hours—often 48 hours—to monitor heart rate and blood pressure.
Another group of infants for whom caution is needed are those with PHACE syndrome. (PHACE is an acronym representing posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and other cardiac defects and eye abnormalities (Ophthalmology. 1999;106(9):1739-1741).) Dr. Drolet cited a study reporting that about one-third of infants with large infantile hemangiomas of the head and neck have PHACE syndrome, and these infants have a congenital vasculopathy that may put them at higher risk for some of propranolol’s side effects (Pediatrics. 2010;126(2):e418-e426).
Developing Protocols
Questions still remain regarding propranolol’s mechanisms of action, the best dose to use, the best way to start and stop treatment and why some hemangiomas respond better than others, according to Dr. Buckmiller.
Dr. Buckmiller and her colleagues are currently looking at standardizing a protocol they use at their institution. “There are many ways that different institutions administer propranolol, and we need to come to a consensus,” she said. “As we understand more, our protocols change.”
Since the publication of the 2010 paper in which she and her colleagues described their protocol (Laryngoscope. 120(4):676-681), Dr. Buckmiller said that her institution has already made some minor changes to the protocol to ensure maximum safety.
Overall, Dr. Buckmiller recommended that physicians who have scant experience with using propranolol in this setting get help from institutions with more experience or refer their patients to those institutions.
Leave a Reply