What is the correlation of physiologically important electromyographic (EMG) waveforms with demonstrable muscle activation used for the reliable interpretation of evoked waveforms during intraoperative neural monitoring (IONM) of the vagus nerve, recurrent laryngeal nerve (RLN), and external branch of the superior laryngeal nerve (EBSLN) in thyroid surgery?
Bottom line
Target musculature is the primary innervated muscle that produces the highest EMG amplitude and is the sole muscle grossly contracting with nerve stimulation.
Explore This Issue
March 2017Background: IONM provides additional functional information during thyroid surgery. Confusion in interpretation of IONM data can ensue when intraoperative EMG waveforms are recorded in isolation from true demonstrable muscular response. Direct stimulation of local muscle fibers with resultant regional contraction could be confused with neural stimulation of a branch of the RLN or EBSLN if EMG morphology is not interpreted correctly.
Study design: Retrospective chart review of 50 surgical sides from 37 thyroid surgery patients with laryngeal nerve IONM from January to December 2015.
Setting: Massachusetts Eye and Ear Infirmary, Boston.
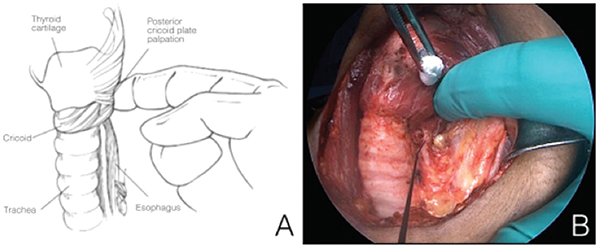
Figure 1. A) Laryngeal twitch can be palpated with a finger placed on the posterior aspect of the larynx during recurrent laryngeal nerve (RLN) or vagal stimulation. B) Stimulator probe points to the left RLN in the photo.
Credit: Copyright 2016 The American Laryngological, Rhinological and Otological Society, Inc.
Synopsis: The target muscle for vagal/RLN stimulation was the ipsilateral vocalis muscle, based on large EMG amplitudes and laryngeal twitch presence (see Figure 1). The target muscle for EBSLN stimulation was the ipsilateral CTM, based on large EMG amplitudes and correlated muscular contraction. In contrast, non-target muscle groups showed small EMG amplitudes and a concomitant lack of muscular contraction. With vagal/RLN stimulation, mean target ipsilateral vocalis EMG amplitude response for all 50 sides was 1,095.7 µV; non-target muscle groups showed much smaller EMG amplitudes, with a mean of 304.0 µV (ipsilateral CTM), 281.6 µV (contralateral vocalis), 45.3 µV (contralateral CTM), and 17.7 µV (ipsilateral straps). With EBSLN stimulation, mean target ipsilateral CTM EMG amplitude response for all 50 sides was 6,379.3 µV; mean amplitudes for non-target muscle groups were 156.73 µV (ipsilateral vocalis), 85.4 µV (contralateral vocalis), 65.0 µV (contralateral CTM), and 17.0 µV (ipsilateral straps). The large-amplitude EMG response of the target muscle for both the vagus/RLN and EBSLN systems was correlated with a meaningful muscular response through visualization and/or palpation of target muscle activation, in stark contrast to a lack of any visual or palpable nontarget muscle activation.