By now, you’re probably well versed in the clinical aspects of the health reform bill signed by President Obama in March. But what you may not know is that the bill includes a section that could benefit otolaryngologists and other physicians in their role as employers.
Explore This Issue
July 2010Beginning this tax year, the bill offers small businesses tax credits to purchase health insurance for their employees. But the Patient Protection and Affordable Care Act also includes penalties for businesses that have 50 or more employees and don’t provide coverage.
The tax credit provisions are a positive development for some physician practices, said Allison Brown, a government affairs representative for the Medical Group Management Association (MGMA). “Like an employer in any industry, physicians are more competitive if they’re able to offer health care coverage, and if this helps a business thinking about dropping coverage because of the rise in costs to retain insurance, then it certainly is a benefit,” Brown said.
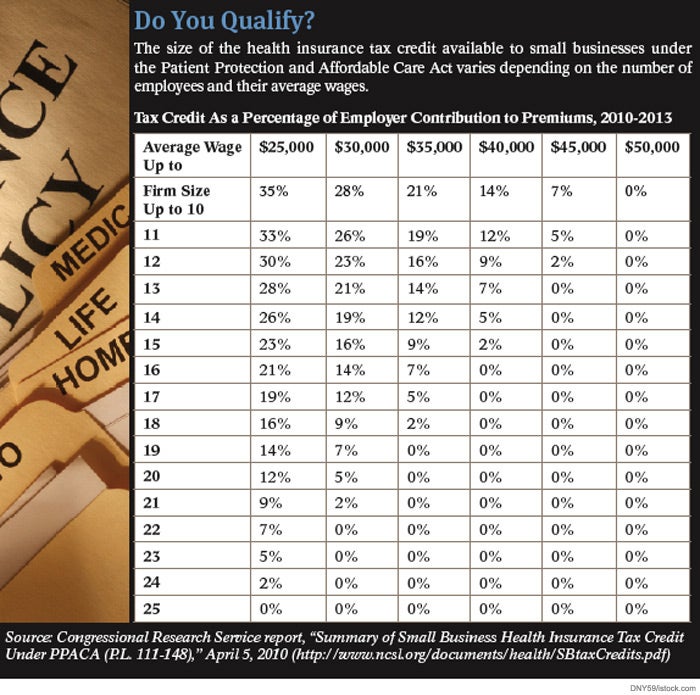
But there are stipulations. To qualify, businesses must cover at least 50 percent of employees’ premium costs. A credit is only available to employers with fewer than 25 full-time equivalent employees (FTEs) earning average wages of less than $50,000 annually. The maximum credit of 35 percent of employers’ share of premiums is available to businesses with fewer than 10 FTEs with average wages of less than $25,000 a year.
When calculating the number of FTEs, practices can include part-time workers, according to Internal Revenue Service guidance. To determine the number of FTEs, a business must first add up the number of hours for which it pays wages to employees during the year; however, the figure cannot exceed 2,080 hours for any given employee. The total is then divided by 2,080.
The credit is retroactive to January 2010 and lasts in this form through 2013. In 2014 and 2015, the size of the credit jumps to 50 percent of employers’ premium contributions, but, in order to qualify, businesses must purchase coverage through the state health insurance exchanges slated to begin in 2014.
Wage Requirements
Many small physician practices would be eligible for the credit based on number of employees, but the wage restriction could rule out some of them, Brown said. Although physician owners’ salaries aren’t factored into the average wage calculation, employed physicians’ salaries are. Employed doctors make well above $50,000 a year and could put average employee wages above that mark, Brown says. In addition, doctors often employ highly trained staff, such as nurse practitioners, whose earnings are frequently above the law’s limit.
Kelly Ladd, chief operating officer for Northwest ENT in Marietta, Ga., says the wage requirements likely will make the practice ineligible for a tax credit because two of the practice’s four doctors are employed and two audiologists are on staff.
A small tax credit might not make a big difference to physician practices if premiums keep rising at double-digit rates, Ladd said. Northwest ENT’s premiums rose 17 percent last year.
It’s too early to tell how otolaryngologists and other small businesses might react in 2014, when the tax credits are only available to small businesses buying coverage in the state insurance exchanges, Brown said. “We’ll have to wait and see when we’re a little bit closer to understanding how the exchanges are going to work,” she said. The credits could provide a powerful incentive to buy on an exchange, both Brown and Ladd said.
“As an employer, if I can insure my employees and do it as inexpensively as possible because my bottom line is shrinking and I need to make up the shortfall somewhere, then I’ll go with the exchange,” said Ladd, who is president of the Association of Otolaryngology Administrators (AOA). “The employees might not like it, but if it’s going to be cheaper, you would be crazy not to.”
Provisions in the law that create penalties by 2014 for businesses that don’t offer health insurance are causing some concern in the medical community. The fee is $2,000 per full-time employee for businesses that employ 50 or more workers and do not offer coverage and that have at least one full-time employee who receives a premium tax credit under the law, according to the Kaiser Family Foundation. The first 30 employees are excluded from the assessment.
Most physicians already provide coverage, Ladd said. The AOA’s 2009 annual salary survey found that 96.7 percent of responding practices offered health insurance and that the mean percentage of the cost paid by a practice was nearly 84 percent. But, Ladd said, “I’m hearing more and more people saying, ‘We just can’t afford to offer health insurance anymore.’”
About 80 percent of AOA members are in one- or two-doctor practices, which likely wouldn’t hit the 50-employee threshold for facing a penalty, Ladd notes. About 15 percent of members are in practices of four to 10 doctors, which, at the higher end, could have 50 workers depending on whether ancillary services, such as audiology, CT scans and allergy care, are provided. The remaining 5 percent of members employ more than 10 doctors.
The new reform law also contains a provision mandating that insurers cover dependents up to age 26 on their parents’ insurance plans. The MGMA has received a lot of calls from physicians who are parents of older children who might qualify when the requirement begins in September, Brown said. “They want to know if they can take advantage of that,” she added.
Leave a Reply