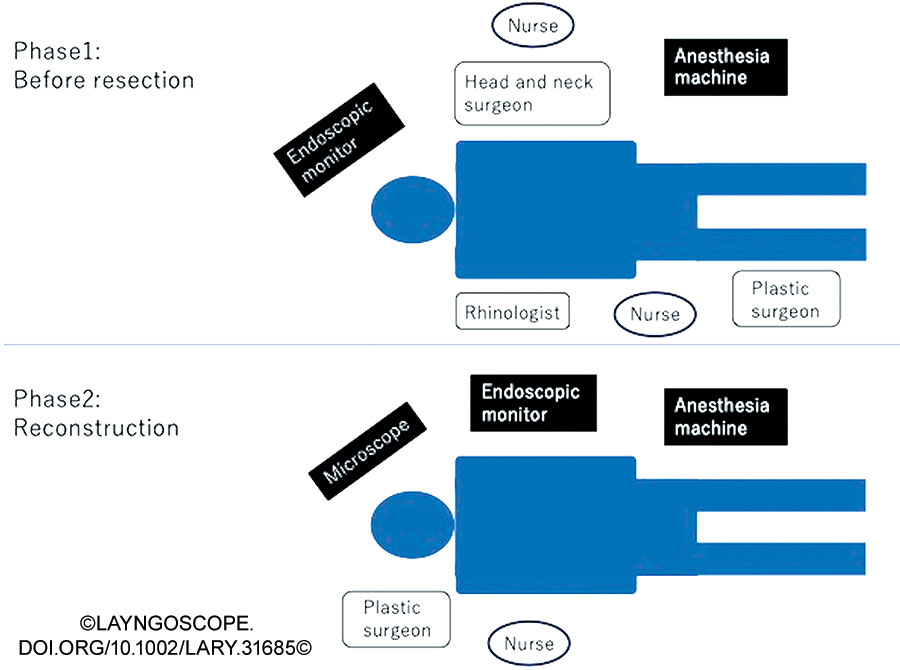
Figure 1: Intra-operative setting. Before resection: The otolaryngologist stands on the patient’s right side, with the endoscopic monitor on the head side. When operations can be performed simultaneously, the head and neck surgeon stands to the left of the patient to operate. The reconstructive surgeon also performed the surgical operation at the same time as the resection physician. Reconstruction: The reconstructive surgeon stands at the patient’s head side to operate.\
Surgical Technique
Explore This Issue
June 2025A three-dimensional model (LEXI Corporation, Tokyo, Japan) of the facial bone was created prior to surgery. Information on the extent of resection was shared between the head and neck surgery and plastic surgery teams. Considering the tumor location, a surgical passage through the nasal septum was created from the contralateral nasal cavity. An additional surgical passage through the anterior wall of the maxillary sinus was created if the anterior wall was not invaded. For lesions occupying the maxillary sinus, a transconjunctival approach was used with an eyelid conjunctival incision.
The contralateral sinus was opened during endoscopic manipulation. A nasal septal mucosal flap was created and preserved. The anterior wall of the sphenoid sinus was opened through the transnasal septum. The Draf III was performed, and the frontal sinuses were opened on both sides. The nasal septal cartilage was removed to widen the working space inside the nasal cavity on the lesion side. The pyriform aperture was exposed, and the nasolacrimal duct was dissected (Fig. 2A). The periorbita was exposed so as not to touch the tumor protruding into the nasal cavity. To reduce the operative time, endoscopic manipulation and oral incision were performed simultaneously. The anterior wall of the left maxilla was exposed, and the bone was exposed to the maxillary zygomatic ridge. Intraorally, a mucosal incision was made in the hard palate mucosa and around the pterygoid process, and the mandibular muscle process was removed. An eyelid conjunctival incision was made to reveal the orbital rim and expose the anterior wall of the maxillary sinus. The orbital rim and pyriform aperture were identified, and the nasal bone was cut endoscopically (Fig. 2B). The bone of the orbital floor was exposed, and the zygomatic process was cut with a bone saw with endoscopic assistance (Fig. 2C). The bone was exposed after a mucosal incision was made at the base of the nasal cavity. The median part of the hard palate was severed endoscopically, and the borders between the soft and hard palates and the Eustachian tube were also separated (Fig. 2D). The Vidian nerve was identified at the pterygoid base, the sphenopalatine artery was cauterized, and the pterygoid base was shaved from the nasal side (Fig. 2E). Subsequently, the tumor gained mobility, the residual pterygoid muscle was resected, and the mass was removed en bloc. The orbital floor was replaced with a titanium plate, and the maxillary defect was reconstructed with a free fibula. Excess bone protruding into the nasal cavity was shaved and adjusted endoscopically. Finally, the exposed bone was covered with a nasal septal mucocutaneous valve (Fig. 2F).
Leave a Reply