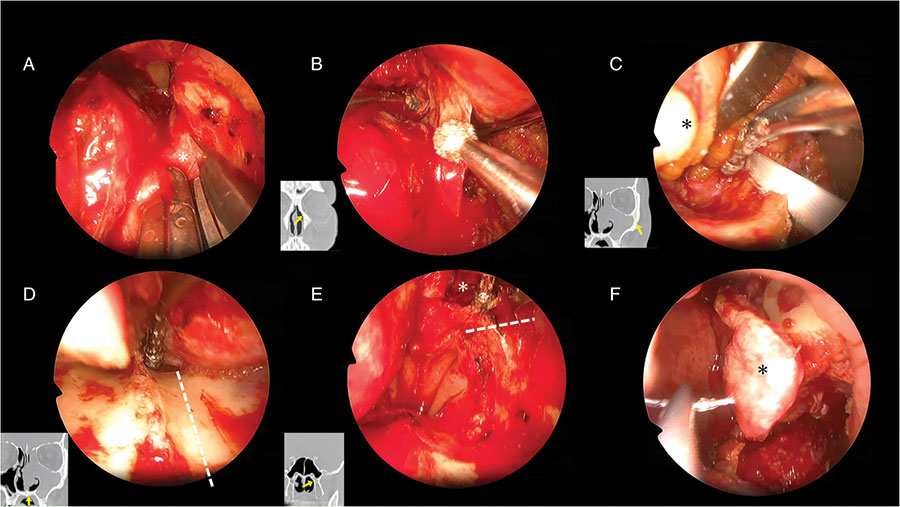
Figure 2: Nasal endoscopic surgical findings. (A) Findings in the left nose after nasal septal cartilage removal and right endoscopic surgical manipulation. The nasolacrimal duct at the medial wall of the orbit was cut (asterisk). (B) The orbital rim and pyriform aperture were identified, and the nasal bone was cut. (C) The bone of the orbital floor was exposed and cut with a bone saw while avoiding intraorbital fat (asterisk). (D) The bone was exposed on the nasal floor. The hard palate was endoscopically shaved and cut (dotted line). (E) The sphenoid sinus was open (asterisk). The base of the pterygoid process was drilled (dotted line). (F) The exposed fibula in the nasal cavity was endoscopically covered with a nasal septal mucocutaneous valve (asterisk).
RESULTS
Regarding endoscopic manipulation, a maximal three-port approach was used in Cases 1 and 2 to perform subtotal maxillectomy (Fig. 3). Case 3 involved a lesion occupying the maxillary sinus (Fig. 4); the zygomatic process was cut via two ports and a transconjunctival approach. A gingival incision was also made in all cases. In all cases, the tumor protruding into the nasal cavity was identified endoscopically and removed as one lump without incision.
Explore This Issue
June 2025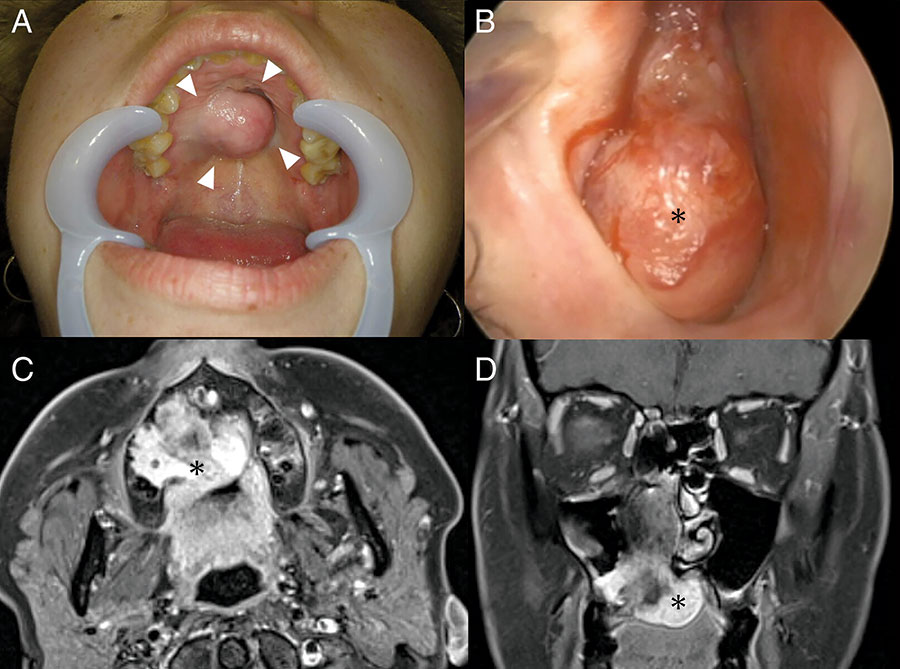
Figure 3: Pre-operative imaging findings of Case 1. (A) Pre-operative intraoral findings. Tumor (arrow) bulge centered on the hard palate. (B) Right nasal findings. It was filled with a tumor (asterisk). (C) Magnetic resonance imaging (MRI; contrast-enhanced T1-weighted image, horizontal section). An internally heterogeneous tumor (asterisk) with partial contrast was observed, destroying the hard palate. (D) MRI (contrast-enhanced T1-weighted image, coronal section). A tumor (asterisk) was found in the nasal cavity, destroying and invading the hard palate. The tumor had partly extended into the interior of the maxillary sinus.
Case 1 was histopathologically diagnosed as myoepithelial carcinoma, and Cases 2 and 3 as squamous cell carcinoma, with negative resection margins in all cases, and no additional treatment required. The immediate post-operative and two-month post-operative facial appearances in Case 3 are shown (Fig. 5). The facial appearance and intranasal and oral findings of patients in cases 1 and 2 after surgery are shown (Fig. 6). No facial skin incisions were present, and patients were satisfied with the post-operative cosmetic outcomes. In all cases, the nasal cavity was covered with a mucous membrane, and there was minimal crusting.

Figure 5: Photographs of Case 3 immediately after surgery (A–C) and two months after surgery (D–F). (A) The patient underwent a subconjunctival eyelid incision. After surgery, mild eyelid hyperemia and internal hemorrhage were observed. (B) The defect was reconstructed using a skin island obtained simultaneously with the fibula. (C) The tumor was resected in one lump, together with a tumor protruding medially into the nasal cavity. (D) Facial findings two months after surgery show no skin incision on the face. The lower eyelid is slightly retracted. (E) Contralateral inferior nasal dorsum (asterisk); a skin island (arrow) can be seen in the nasal cavity. A nasal septal valve (arrowhead) is used, and the interior of the nose is covered with a mucous membrane. (F) 3D CT imaging. The orbital floor was reconstructed with a titanium plate, and the interior of the maxillary sinus with fibula.
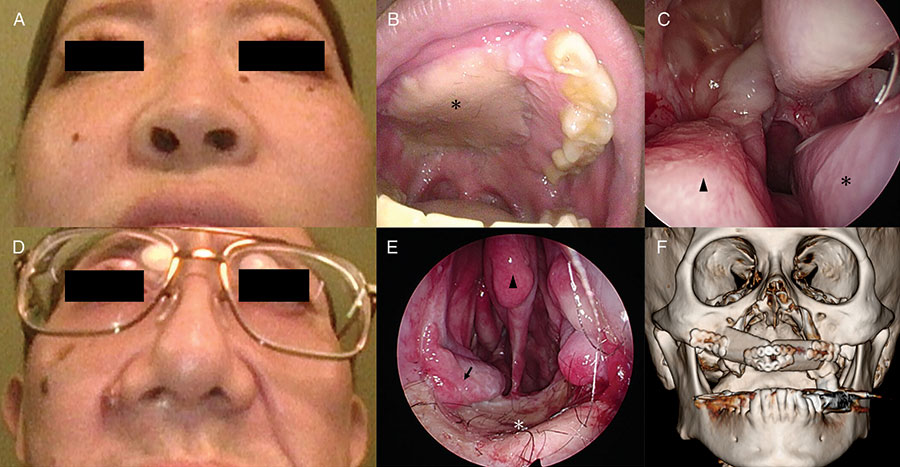
Figure 6: Photographs of Case 1, eight months after surgery (A-C) and Case 2, seven months after surgery (D-F). (A) Facial findings eight months after surgery show no skin incision on the face. (B) The defect was reconstructed using a skin island obtained simultaneously with the fibula. Skin islands (asterisk) conform to the surrounding tissue. (C) Contralateral inferior nasal dorsum (asterisk). A nasal septal valve (arrowhead) is used, and the interior of the nose is covered with a mucous membrane. (D) Facial findings seven months after surgery show no skin incision on the face. (a) The defect was reconstructed using a skin island obtained simultaneously with the fibula. Skin islands (asterisks) replace the nasal floor. Nasal septum removed, only the upper part (arrowhead) remaining. A nasal septal valve (arrow) is used, and the interior of the nose is covered with a mucous membrane. (F) 3D CT imaging. The orbital floor was reconstructed with a titanium plate, and the interior of the maxillary sinus with fibula. Most of the hard palate and the right maxillary sinus defect have been replaced by fibula.
Leave a Reply