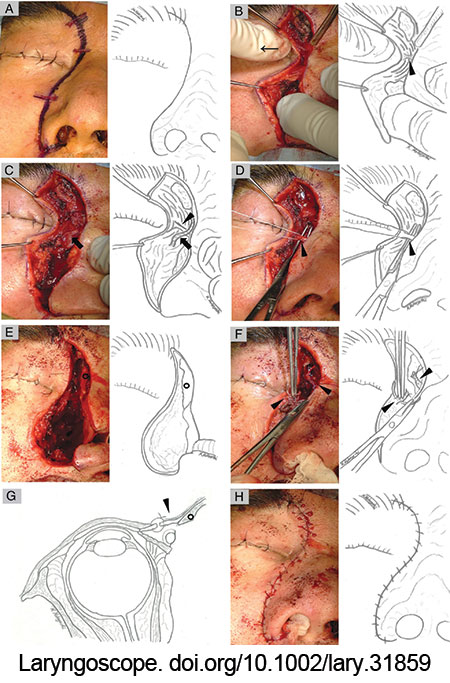
Figure 1: Intra-operative photograph of right medial maxillectomy via lateral rhinotomy. The head was at the top of the photograph. (A) Lateral rhinotomy incision begins at the inferior hairline of the eyebrow. (B) By pulling the eyelashes laterally (thin arrow), the MPL stood out in a shallow layer. (C, D) The anterior limb of the MPL (arrowhead) was identified just below the angular vein (arrow). (E) The osteotomy spared the frontal process of the maxilla and the nasal bone (black circle). (F, G) The anterior rim of the MPL (arrowhead) was repaired with a ligament-to-ligament suture. (H) Skin sutures were formed meticulously.
RESULTS
Pathologically, there were three patients with olfactory neuroblastoma, two patients with human papillomavirus-related multiphenotypic sinonasal carcinoma, one patient with squamous cell carcinoma, and one patient with adenocarcinoma. The primary tumor was resected via a medial maxillectomy in three patients and craniofacial resection with medial maxillectomy in four patients. Medial maxillectomy was performed via a lateral rhinotomy in all patients. Three of the four patients who required craniotomy underwent free flap reconstruction. Three patients required resection of the orbital periosteum and reconstruction with fascia lata. The median follow-up period was 23 months (range, 12–68 months). The MPL was identified in all patients. The median time from skin incision to MPL tagging was 13 min (range, 11–25 min). Ligament-to-ligament suture of the anterior rim of the MPL was achieved in six patients; however, in one patient, the ipsilateral frontal process of the maxilla and nasal bone were completely resected due to tumor invasion; ligament-to-ligament suture of the MPL was difficult. In this case, the lateral cut end of the ligament was sutured to the medial subcutaneous tissue at the same height. All patients underwent surgery as planned, with negative resection margins. The patient with unsuccessful ligament-to-ligament suture of the MPL experienced inner canthus malposition post-operatively (Fig. 2).
Explore This Issue
March 2025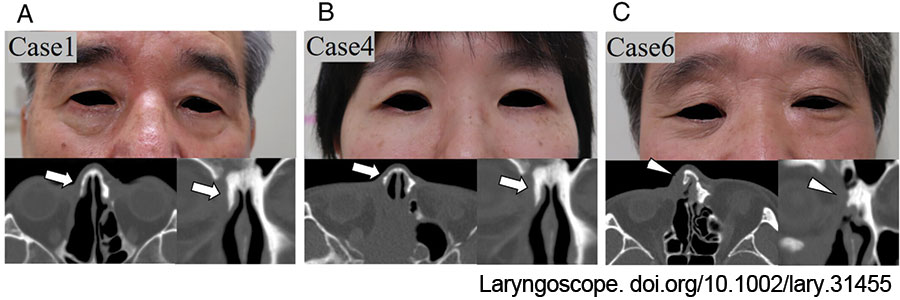
Figure 2: Post-operative facial photographs and CT images. (A, B) Patients 1 and 4 had normal canthal position post-operatively. The frontal process of the maxilla and nasal bone were partially preserved (arrows). The MPL was repaired with a ligament-to-ligament suture. (C) Patient 6 had canthus malposition post-operatively. The ipsilateral frontal process of the maxilla and nasal bone were resected (arrowheads). As a result, ligament-to-ligament suturing of the MPL was unsuccessful. doi.org/10.1002/lary.31859
CONCLUSION
The MPL is easily identified with the eyelash traction test. The angular vein is an anatomical marker. To prevent post-operative canthus malposition, it is important to perform an osteotomy that preserves the frontal process of the maxilla and the nasal bone and to ensure MPL repair with a ligament-to-ligament suture.