 TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope articles free of charge, visit Laryngoscope.
TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope articles free of charge, visit Laryngoscope.
Explore This Issue
May 2021Introduction
Endoscopic endonasal surgery (EES) is performed through a narrow corridor by inserting an endoscope and surgical instruments from the nostril. Securing an adequate working space is thus crucial to manipulating both the endoscope and instruments without conflict. To secure the working space for any type of EES, a large sphenoidotomy with wide opening of the anterior wall of the sphenoid sinus is a crucial step.
The Vidian canal is a well-known landmark for the lacerum carotid artery and is also known as a lower lateral limit in anterior sphenoidotomy (J Neurosurg. 2008;108:177-183). However, localizing the Vidian canal is sometimes difficult in the clinical setting of EES. The palatovaginal canal (PVC) is a bony tunnel formed by the upper edge of the sphenoid process of the palatine bone and the vaginal process of the sphenoid bone that connects the nasopharynx with the pterygopalatine fossa (AJR Am J Roentgenol. 2002;179:267-272). The PVC contains the pharyngeal nerve (PN) and the pharyngeal artery (PA). The PN is a neural branch from the supramaxillary nerve via the pterygoid ganglion, and is thought to be associated with sense of the nasopharynx. The PA is a branch of the maxillary artery and anastomoses with the ascending pharyngeal artery (AJNR Am J Neuroradiol. 1996;17:1148-1150). The PVC is a landmark for the Vidian canal due to its location just medial to the canal, projecting mediocaudally (Laryngoscope. 2012;122:6-12). Appearing as a hole, the PVC can be the first recognized object seen when detaching the nasal septal mucosa laterally and inferiorly from the vomer and sphenoid bone (J Neurol Surg B Skull Base. 2012;73:352-357).
Several studies have described the anatomy of the PVC from computed tomography (CT) scans or cadaveric specimens (AJR Am J Roentgenol. 2002;179:267-272; AJNR Am J Neuroradiol. 1996;17:1148-1150; Laryngoscope. 2012;122:6-12; J Neurol Surg B Skull Base. 2012;73:352-357), but opening the PVC in clinical cases has not been reported in localizing the Vidian canal and maximizing the sphenoidotomy.
Method
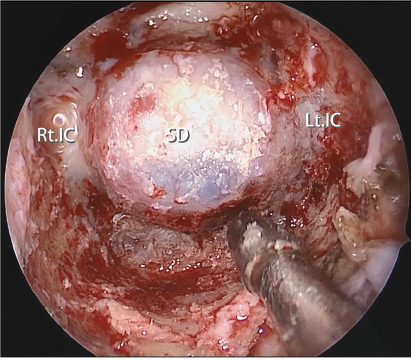 Fig. 1. Final endoscopic view after resection of the anterior wall of the sphenoid sinus including the PVC to the medial edge of the Vidian canal. Note the inferolateral part of the anterior sphenoidotomy is maximized, expanding the working corridor for surgical instruments. SD = sellar dura; Lt. IC = left internal carotid artery; Rt. IC = right internal carotid artery.
Fig. 1. Final endoscopic view after resection of the anterior wall of the sphenoid sinus including the PVC to the medial edge of the Vidian canal. Note the inferolateral part of the anterior sphenoidotomy is maximized, expanding the working corridor for surgical instruments. SD = sellar dura; Lt. IC = left internal carotid artery; Rt. IC = right internal carotid artery.