INTRODUCTION
In recent years, the treatment of Zenker’s diverticulum (ZD) and other hypopharyngeal diverticula has undergone substantial transformation. Refinement in instrumentation and surgical technique have led to improvements in treatment outcomes and treatment-associated morbidity. Flexible endoscopic Zenker’s surgery has gained wider acceptance and has resulted in the ability to treat more patients with these disorders using minimally invasive endoscopic techniques previously relegated to only open approaches. Although gastroenterologists with training in advanced endoscopy have been performing tunneled peroral endoscopic myotomy over the past decade, few otolaryngologists and thoracic surgeons have been exposed to flexible endoscopic surgery in their training.
Explore This Issue
March 2025Flexible Zenker’s surgery is not a new phenomenon. The initial techniques described by Brazilian and Dutch groups in the mid-1990s used a flexible gastroscope with electrosurgical instruments fed through a working channel to simply divide the common wall or septum in a procedure called a standard septotomy. During the early days of the standard septotomy, a centimeter or more of the common wall was left undivided as a precaution against esophageal leaks; however, a 2013 series of 150 patients treated with standard septotomy reported short-term improvement in dysphagia symptoms but also found a 20% recurrence rate.
The Z-peroral endoscopic myotomy (Z-POEM) was developed to address the issue of recurrence while providing a safe post-operative result that minimized leaks. The submucosal tunneling (“third space” endoscopic surgery) and endoscopic myotomy techniques classically used at the lower esophageal sphincter for endoscopic achalasia treatment were adapted to the upper esophageal sphincter.
Our objective is to provide a path for otolaryngologists not familiar with advanced flexible endoscopic surgical techniques to build on their existing skills with rigid diverticulotomy to eventually gain the ability to perform a purely flexible Zenker’s surgery for patients who prefer an endoscopic approach but have anatomic factors that prohibit rigid exposure and comorbidities that preclude open surgery. Just as with rigid diverticulotomy surgery, the surgical goals are the same: to fully perform a cricopharyngeus muscle myotomy and divide the common wall so a food bolus will continue to flow distally during the swallow.
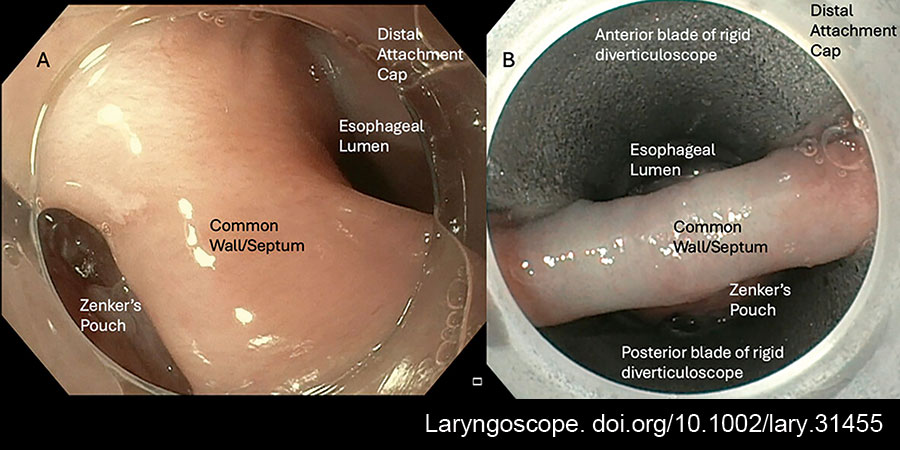
Figure 1: Image (A) shows the endoscopic view of the common wall through the Olympus H190 gastroscope with distal attachment cap; the diverticulum is to the left of the common wall and the esophageal lumen is to the right. Image (B) shows the common wall of the diverticulum exposed through a bivalved diverticuloscope with the esophageal lumen above and the diverticulum below the common wall. doi.org/10.1002/lary.31455