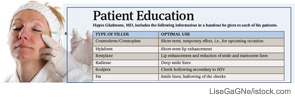
With the availability of noninvasive procedures that use injectable fillers to do the work surgery once monopolized, more people than ever before are seeking the elixir of youth that comes now at the end of a needle rather than a knife.
With the availability of noninvasive procedures that use injectable fillers to do the work surgery once monopolized, more people than ever before are seeking the elixir of youth that comes now at the end of a needle rather than a knife.

Otolaryngologists are likely to see some changes in the way informed consent is handled at the hospitals where they perform surgery. Recent changes from the Centers for Medicare and Medicaid Services (CMS), along with Joint Commission rules, have prompted many hospitals and health systems to get more involved in what previously fell firmly in the physician’s purview.
Hayes Wanamaker, MD, an otolaryngologist in Syracuse, N.Y., refers to the recovery audit process of insurance carriers as the proverbial camel’s nose under the tent.
When Rahul Shah, MD, then a pediatric otolaryngologist at Children’s Hospital in Boston, and several colleagues first undertook a survey of otolaryngologists’ reactions to adverse events in 2004, they provided a blank form for respondents to write about what had happened. In the more than 200 responses they received, Dr. Shah and his colleagues read an outpouring of emotion.

By now, you’re probably well versed in the clinical aspects of the health reform bill signed by President Obama in March. But what you may not know is that the bill includes a section that could benefit otolaryngologists and other physicians in their role as employers.

Dr. Roberts used numbers to illustrate his point during a presentation at the Annual Meeting of the American Broncho-Esophagological Association, part of the Combined Otolaryngological Spring Meetings held here April 28-May 2.

Are you looking to switch medical practices? Are you in the market to purchase a professional malpractice insurance policy? Are you planning to retire soon? If you answered ‘yes’ to any of these questions, you will likely confront the concept of “tail” insurance.

The new health system reform law includes a number of quality provisions that physician organizations say are not ready for primetime and won’t be ready in the time frame established by Congress.
I have been a strong advocate of electronic medical records (EMRs) for almost a decade. In fact, I used the phrases “It is the silver bullet for health care reform infrastructure” and “It is the cornerstone for health care reform infrastructure” to describe EMR plans when President Obama was campaigning. However, technology, like fire, can warm your house or burn it down, cook your food or kill you. Likewise, the wrong EMR will escalate inefficiency and raise health care costs. The wrong mandates or the wrong incentives have the potential to paralyze the day-to-day practice of medicine.

The federal government’s proposed rule establishing incentive payments for physicians who “meaningfully use” electronic health records (EHRs) is too onerous and would discourage physicians from participating, some otolaryngologists say.