Over the past few decades, a transition toward culture-directed antibiotics has shifted the treatment paradigm of SBO toward primary medical management, with mortality rates now decreasing to 10-20% compared to 50% initially.

Over the past few decades, a transition toward culture-directed antibiotics has shifted the treatment paradigm of SBO toward primary medical management, with mortality rates now decreasing to 10-20% compared to 50% initially.
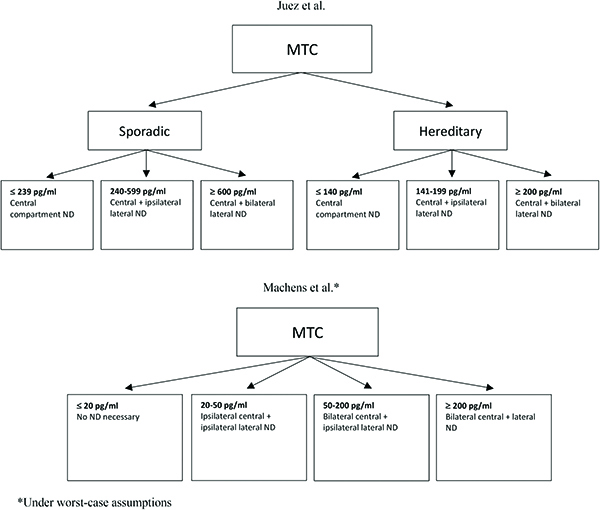
Medullary thyroid carcinoma (MTC) comprises less than 5% of thyroid cancers but is responsible for more than 10% of deaths related to thyroid cancer.
Antithrombotic management is a key component of surgical optimization, as it necessitates balancing the risk of a peri-operative thrombotic event with the risk of bleeding.
The use of p16 as a surrogate marker for HPV has gained traction, but is it sufficient as a surrogate for HPV-related squamous cell carcinoma?
Most current literature suggests that cefazolin is safe for surgical prophylaxis in patients with penicillin allergy.
Multimodal pre-habilitation and rehabilitation have been an important topics in the literature, aiming to combat modifiable patient factors like sarcopenia, malnutrition, and psychological status.
Resectable stage IVA/IVB tumors should be treated with surgery followed by chemoradiation, with consideration for dabrafenib/trametinib biotherapy for BRAFV600E-mutated tumors.
Nuclear medical imaging is strongly recommended in the diagnosis of paragangliomas that are familial, SDHB variants, malignant, or potentially multifocal, but those that have classic presentations do not routinely require peptide receptor imaging.

Sinonasal neoplasms have a wide spectrum of histopathologies and biological behaviors, but close proximity to critical structures, such as the skull base and orbit, can make surgical resection a challenge.
In the era of effective adjuvant systemic therapies, the use of ICI alone in the adjuvant setting may be insufficient to effectively reduce regional failure.