“When we went to our EMR system three years ago, I had to spend a tremendous amount of time learning how the system worked and less [time] actually talking to patients,” said Michael Setzen, MD, clinical associate professor of otolaryngology at New York University School of Medicine and a physician in private practice in Great Neck, N.Y. “They weren’t happy that I was in the room with them using the computer. Overall, the volume of interactions with patients will be decreasing. For how long is the major question.”
Explore This Issue
December 2011Audit Workflows
Another thing practices should undertake soon is a top-to-bottom workflow audit.
“We are telling clients they should inventory the practice looking for any use of ICD-9 codes on superbills, forms, policies, reports and payer information,” said Pollock. “Run a frequency report to determine your top 25 or so diagnosis codes. Then you can map the ICD-9 codes to the draft ICD-10 codes now. Look for areas of insufficient documentation to choose the appropriate ICD-10 code. Then, when the final code set is released in October 2013, you are a step ahead in ensuring your documentation will support the new codes.”
Every part of your practice will need to be assessed. At the front desk, privacy policies will most likely need revisions, as will patient encounter systems. The practice managers will have to look at all policies and procedures associated with a disease code, disease management, tracking and the Physician Quality Reporting Initiative while also reviewing and updating all vendor and payer contracts. Nursing will be involved in changes to order forms and prior authorizations. Even the laboratory will need to be more precise in how it documents its work.
Training
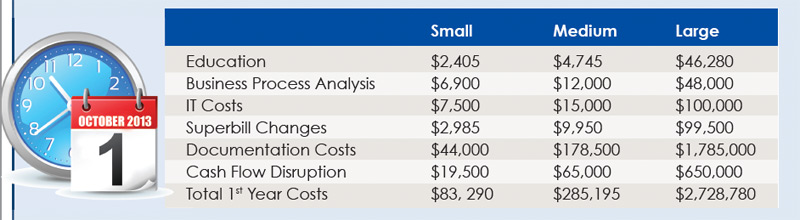
One of the most significant costs to the practice will most likely be staff training. Not only will the coding and billing staffs need to be educated, but the physicians themselves will need training.
Leave a Reply